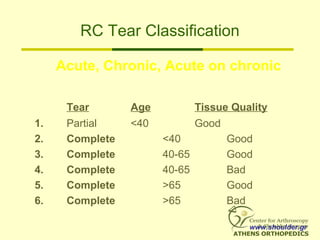
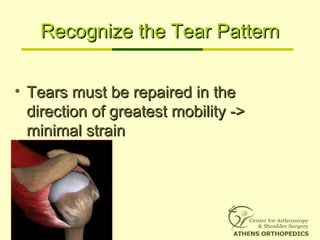
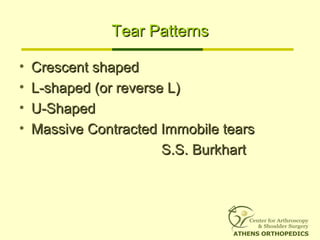
This document discusses techniques for repairing rotator cuff tears arthroscopically. It begins by describing the classification of partial versus full thickness tears and massive tears involving two or more tendons. For massive contracted immobile tears, interval slides can be performed through the anterior and posterior intervals to regain mobility. Repair techniques depend on the tear pattern, such as side-to-side sutures for U-shaped tears or interval slides for massive immobile tears. Results of arthroscopic repair for massive tears show 84-94% excellent or good results according to several studies. The key is to match the repair technique to the tear morphology and mobility to minimize strain on the repair.

![Tears’ Definitions
• Partial Thickness Tears =
absence of communication between the
glenohumeral joint and the subacromial
bursa.
• Full Thickness Tears =
communication between the glenohumeral
joint and the subacromial bursa.
• Massive Tear =
Involving 2 or 3 tendons [Gerber]
or bigger than 5cm [Cofield]
www.shoulder.gr](https://image.slidesharecdn.com/ps6ux8rsstyjx5sxwew0-signature-69d9f1a3cb3f2649714837b93c1c3b7b41f9a67bbef005eecf911e10fcb33758-poli-170927100657/85/Fixation-techniques-in-rot-cuff-repair-4-320.jpg)
![How frequent are RC Tears?
• Rotator Cuff Frequency:
30% of population
• Significant correlation with
age [Sher JS, Arthroscopy 1995]
www.shoulder.gr](https://image.slidesharecdn.com/ps6ux8rsstyjx5sxwew0-signature-69d9f1a3cb3f2649714837b93c1c3b7b41f9a67bbef005eecf911e10fcb33758-poli-170927100657/85/Fixation-techniques-in-rot-cuff-repair-6-320.jpg)
![Natural History of a Tear
• Tears DO NOT HEAL. Some but NOT ALL of them will
progress
• Rot cuff arthropathy is the end stage (4-20%)
• 50% of newly symptomatic tears will progress in size
• 20% of asymptomatic tears will progress.
• No Tear seem to decrease in size.
• 80% of partial tears progress in size or become full
thickness at 2 years
[Yamaguchi K., 2006, Nice Shoulder Course]
www.shoulder.gr](https://image.slidesharecdn.com/ps6ux8rsstyjx5sxwew0-signature-69d9f1a3cb3f2649714837b93c1c3b7b41f9a67bbef005eecf911e10fcb33758-poli-170927100657/85/Fixation-techniques-in-rot-cuff-repair-7-320.jpg)
![Partial Tears Treatment Options
1. Debride partial tear only
2. In-situ Repair
3. Convert to full thickness, Debride, Repair
Etiology makes the decision!!!
• Because most tears are degenerative, option 3
should be the best for most cases
• Trauma or young athletes are candidates for in-situ
repair
• If minimal partial tears cause significant pain then
debridement alone
[Yamaguch K, 2006 Nice Shoulder Course]
www.shoulder.gr](https://image.slidesharecdn.com/ps6ux8rsstyjx5sxwew0-signature-69d9f1a3cb3f2649714837b93c1c3b7b41f9a67bbef005eecf911e10fcb33758-poli-170927100657/85/Fixation-techniques-in-rot-cuff-repair-9-320.jpg)




![What to do???
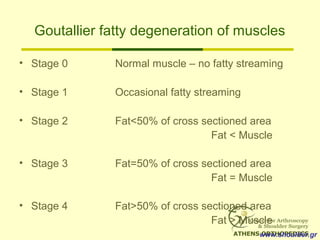
• Patients with grade 3 or 4 fatty degeneration
DO NOT improve with rot cuff repair
[Goutallier]
Vs.
• Patients with grade 3 or 4 fatty degeneration
improved significant at 86% of cases after
arthroscopic repair
[Burkhart]
www.shoulder.gr](https://image.slidesharecdn.com/ps6ux8rsstyjx5sxwew0-signature-69d9f1a3cb3f2649714837b93c1c3b7b41f9a67bbef005eecf911e10fcb33758-poli-170927100657/85/Fixation-techniques-in-rot-cuff-repair-17-320.jpg)
![Our Results
• 41 pts single row repair
• Small 3 (7.31%)
• Medium 26 (63.41%)
• Large 5 (12.18%)
• Massive 7 (17.7%)
• Mean age 58.8 years
• Mean FU 14 months
• UCLA score
Excellent 10 (24.39%)
Good 20 (48.78%)
Fair 9 (21.95%)
Poor 2 (4.87%)
92% Substantial Improvement
in Pain
[Acta Orthopedica Hellenica, 2007]
www.shoulder.gr](https://image.slidesharecdn.com/ps6ux8rsstyjx5sxwew0-signature-69d9f1a3cb3f2649714837b93c1c3b7b41f9a67bbef005eecf911e10fcb33758-poli-170927100657/85/Fixation-techniques-in-rot-cuff-repair-25-320.jpg)























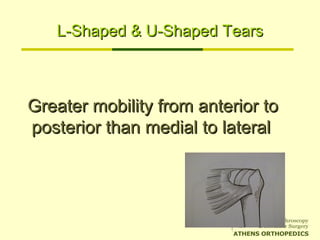
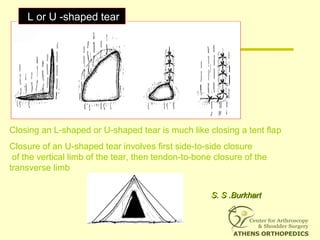
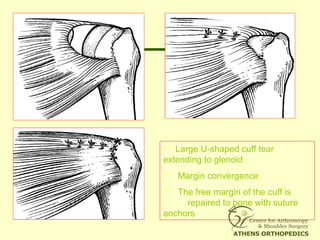
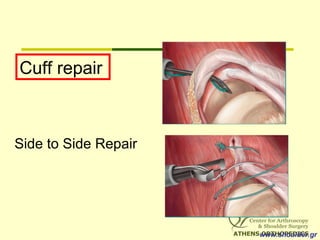
![L-Shaped & U-Shaped TearsL-Shaped & U-Shaped Tears
• Side to side sutures from medial to lateralSide to side sutures from medial to lateral
• Progressively converge the margin of theProgressively converge the margin of the
tear lateral to bone bedtear lateral to bone bed
• Closing 50% of a U-Shaped tear ->Closing 50% of a U-Shaped tear ->
reduces strain at converge margin by areduces strain at converge margin by a
factor of 6factor of 6
[[S. S .Burkhart]S. S .Burkhart]](https://image.slidesharecdn.com/ps6ux8rsstyjx5sxwew0-signature-69d9f1a3cb3f2649714837b93c1c3b7b41f9a67bbef005eecf911e10fcb33758-poli-170927100657/85/Fixation-techniques-in-rot-cuff-repair-73-320.jpg)

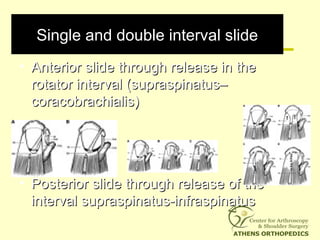
![Massive Contracted Immobile TearsMassive Contracted Immobile Tears
• No mobility from medial to lateral or fromNo mobility from medial to lateral or from
anterior to posterioranterior to posterior
• Subcategories:Subcategories:
– Massive Contracted Longitudinal TearsMassive Contracted Longitudinal Tears
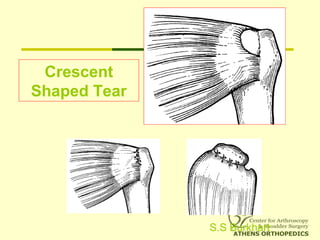
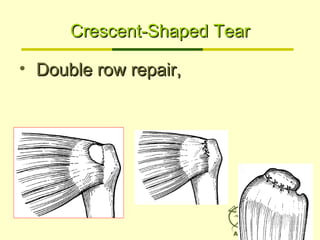
– Massive Contracted Crescent TearsMassive Contracted Crescent Tears
• Represent 9.6% of massive tearsRepresent 9.6% of massive tears
[[S.Burkhart]S.Burkhart]](https://image.slidesharecdn.com/ps6ux8rsstyjx5sxwew0-signature-69d9f1a3cb3f2649714837b93c1c3b7b41f9a67bbef005eecf911e10fcb33758-poli-170927100657/85/Fixation-techniques-in-rot-cuff-repair-79-320.jpg)




![Results for massive tearsResults for massive tears
• 95% Good to Excellent Results95% Good to Excellent Results
independent to tear sizeindependent to tear size [Burkhart, 2001][Burkhart, 2001]
• With interval slideWith interval slide
• Improve UCLA score (10->28.3)Improve UCLA score (10->28.3)
• Improve Active ROM, StrengthImprove Active ROM, Strength
[Burkhart, 2004][Burkhart, 2004]
• Graft Jacket RepairGraft Jacket Repair
• Improve UCLA score (18->32Improve UCLA score (18->32))
[Snyder, 2008][Snyder, 2008]](https://image.slidesharecdn.com/ps6ux8rsstyjx5sxwew0-signature-69d9f1a3cb3f2649714837b93c1c3b7b41f9a67bbef005eecf911e10fcb33758-poli-170927100657/85/Fixation-techniques-in-rot-cuff-repair-96-320.jpg)
![What to do???What to do???
• Patients with grade 3 or 4 fatty degenerationPatients with grade 3 or 4 fatty degeneration
DO NOTDO NOT improve with rot cuff repairimprove with rot cuff repair
[Goutallier][Goutallier]
Vs.Vs.
• Patients with grade 3 or 4 fatty degenerationPatients with grade 3 or 4 fatty degeneration
improved significant at 86% of cases afterimproved significant at 86% of cases after
arthroscopic repairarthroscopic repair
[Burkhart][Burkhart]](https://image.slidesharecdn.com/ps6ux8rsstyjx5sxwew0-signature-69d9f1a3cb3f2649714837b93c1c3b7b41f9a67bbef005eecf911e10fcb33758-poli-170927100657/85/Fixation-techniques-in-rot-cuff-repair-98-320.jpg)










































![ROTATOR CUFF[4273].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/rotatorcuff4273-221222051719-751991ae-thumbnail.jpg?width=640&height=640&fit=bounds)























































