This document discusses rotator cuff tears, including their indications, treatment options, and results. It provides an overview of rotator cuff anatomy and function. It describes the various types and classifications of rotator cuff tears and discusses the history and evolution of rotator cuff repair techniques. Treatment options are discussed depending on factors like the patient's age, tear size and chronicity. Expected results are outlined based on the pre-operative tissue quality and repair achieved.




![Tears’ Definitions
• Partial Thickness Tears =
absence of communication between the
glenohumeral joint and the subacromial
bursa.
• Full Thickness Tears =
communication between the glenohumeral
joint and the subacromial bursa.
• Massive Tear =
Involving 2 or 3 tendons [Gerbers]
or bigger than 5cm [Cofield]
www.shoulder.gr](https://image.slidesharecdn.com/vdmtfurgstkx7fomydpx-signature-69d9f1a3cb3f2649714837b93c1c3b7b41f9a67bbef005eecf911e10fcb33758-poli-170927100658/85/Rotator-cuff-2008-final-6-320.jpg)
![How frequent are RC Tears?
• Rotator Cuff Frequency:
30% of population
• Significant correlation with
age [Sher JS, Arthroscopy 1995]
www.shoulder.gr](https://image.slidesharecdn.com/vdmtfurgstkx7fomydpx-signature-69d9f1a3cb3f2649714837b93c1c3b7b41f9a67bbef005eecf911e10fcb33758-poli-170927100658/85/Rotator-cuff-2008-final-8-320.jpg)
![Full Thickness Tear
Age Frequency
40-60 4-13%
60-70 20%
70-80 50%
>80 80%
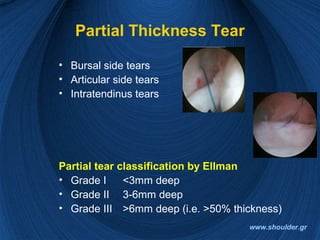
Partial Thickness Tear
Age Frequency
<40 4%
>60 25%
[Tempelhof S, JSES, 1999]
How Frequent are RC Tears?
www.shoulder.gr](https://image.slidesharecdn.com/vdmtfurgstkx7fomydpx-signature-69d9f1a3cb3f2649714837b93c1c3b7b41f9a67bbef005eecf911e10fcb33758-poli-170927100658/85/Rotator-cuff-2008-final-9-320.jpg)
![Bilateral RC Tears
• Rotator Cuff Disease is not only age related,
but also bilateral
• >51% of patients with a previously asymptomatic
rotator cuff tear and a contralateral symptomatic tear
will develop symptoms in the non-symptomatic tear at
the next 2.8 years.
[Yamaguchi K., JSES, 2001]
www.shoulder.gr](https://image.slidesharecdn.com/vdmtfurgstkx7fomydpx-signature-69d9f1a3cb3f2649714837b93c1c3b7b41f9a67bbef005eecf911e10fcb33758-poli-170927100658/85/Rotator-cuff-2008-final-10-320.jpg)

![Natural History of a Tear
• Tears DO NOT HEAL. Some but NOT ALL of them will
progress
• Rot cuff arthropathy is the end stage (4%)
• 50% of newly symptomatic tears will progress in size
• 20% of asymptomatic tears will progress.
• No Tear seem to decrease in size.
• 80% of partial tears progress in size or become full
thickness at 2 years
[Yamaguchi K., 2006, Nice Shoulder Course]
www.shoulder.gr](https://image.slidesharecdn.com/vdmtfurgstkx7fomydpx-signature-69d9f1a3cb3f2649714837b93c1c3b7b41f9a67bbef005eecf911e10fcb33758-poli-170927100658/85/Rotator-cuff-2008-final-12-320.jpg)







![RC Treatment Options
Non-Operative
• 45-80% Satisfactory
Results
BUT
• Symptom resolution ???
• Tear progression ???
• Fatty degeneration ???
• Progression to rot cuff
arthropathy ???
Operative
90% Good to Excellent
Results at 10 years
[Iannotti Wolf]
www.shoulder.gr](https://image.slidesharecdn.com/vdmtfurgstkx7fomydpx-signature-69d9f1a3cb3f2649714837b93c1c3b7b41f9a67bbef005eecf911e10fcb33758-poli-170927100658/85/Rotator-cuff-2008-final-20-320.jpg)

![Grouping the Patients
Group I: patients with minimal risk of
progression to irreversible changes
to the rotator cuff
Group II: patients with high risk of
progression
Group III: patients who have progressed
already
[Yamaguchi K., 2006, Nice Shoulder Course]
www.shoulder.gr](https://image.slidesharecdn.com/vdmtfurgstkx7fomydpx-signature-69d9f1a3cb3f2649714837b93c1c3b7b41f9a67bbef005eecf911e10fcb33758-poli-170927100658/85/Rotator-cuff-2008-final-22-320.jpg)


![Group III patients
• Older than 70 years
– with large or massive tears and
– irreversible damage to the rot cuff
They can benefit from rotator cuff repair,
even a partial repair
www.shoulder.gr
[Yamaguchi K., 2006, Nice Shoulder Course]
[Burkhart, 2007, Arthroscopy]](https://image.slidesharecdn.com/vdmtfurgstkx7fomydpx-signature-69d9f1a3cb3f2649714837b93c1c3b7b41f9a67bbef005eecf911e10fcb33758-poli-170927100658/85/Rotator-cuff-2008-final-25-320.jpg)

![Partial Tears Treatment Options
1. Debride partial tear only
2. In-situ Repair
3. Convert to full thickness, Debride, Repair
Etiology makes the decision!!!
• Because most tears are degenerative, option 3
should be the best for most cases
• Trauma or young athletes are candidates for in-situ
repair
• If partial tear causes significant pain then
debridement alone
[Yamaguch K, 2006 Nice Shoulder Course]
www.shoulder.gr](https://image.slidesharecdn.com/vdmtfurgstkx7fomydpx-signature-69d9f1a3cb3f2649714837b93c1c3b7b41f9a67bbef005eecf911e10fcb33758-poli-170927100658/85/Rotator-cuff-2008-final-27-320.jpg)








![What kind of Repair is
NECESSARY?
• An anatomically deficient RC could be biomechanically
intact rot cuff
[Burkhart]
• Conservative treatment of chronic painful rot cuff tears
will result in a successful outcome in about 50% of
patients
[Cofield]
• Cuff tear arthropathy will develop in 4% of patients with
complete rot cuff tears
[Neer]]
www.shoulder.gr](https://image.slidesharecdn.com/vdmtfurgstkx7fomydpx-signature-69d9f1a3cb3f2649714837b93c1c3b7b41f9a67bbef005eecf911e10fcb33758-poli-170927100658/85/Rotator-cuff-2008-final-36-320.jpg)
![What can we Repair?
• UP to 50% of cuff repairs had a postoperative defect
• This didn’t affected patient satisfaction or pain relief
• But it did affected shoulder strength
[Harryman et all J. B.J.S 1991]
www.shoulder.gr](https://image.slidesharecdn.com/vdmtfurgstkx7fomydpx-signature-69d9f1a3cb3f2649714837b93c1c3b7b41f9a67bbef005eecf911e10fcb33758-poli-170927100658/85/Rotator-cuff-2008-final-37-320.jpg)



![What to do???
• Patients with grade 3 or 4 fatty degeneration
DO NOT improve with rot cuff repair
[Goutallier]
Vs.
• Patients with grade 3 or 4 fatty degeneration
improved significant at 86% of cases after
arthroscopic repair
[Burkhart]
www.shoulder.gr](https://image.slidesharecdn.com/vdmtfurgstkx7fomydpx-signature-69d9f1a3cb3f2649714837b93c1c3b7b41f9a67bbef005eecf911e10fcb33758-poli-170927100658/85/Rotator-cuff-2008-final-41-320.jpg)

![Non-Operative Treatment
Best candidates for non-operative are:
• patients with chronic attritional RC tears
• limited to one tendon
• the onset not associated with significant trauma
• over the age of 60 and less active
[Iannotti J.P.Disorders of the shoulder]
www.shoulder.gr](https://image.slidesharecdn.com/vdmtfurgstkx7fomydpx-signature-69d9f1a3cb3f2649714837b93c1c3b7b41f9a67bbef005eecf911e10fcb33758-poli-170927100658/85/Rotator-cuff-2008-final-43-320.jpg)




















![Our Results
• 41 pts single row repair
• Small 3 (7.31%)
• Medium 26 (63.41%)
• Large 5 (12.18%)
• Massive 7 (17.7%)
• Mean age 58.8 years
• Mean FU 14 months
• UCLA score
Excellent 10 (24.39%)
Good 20 (48.78%)
Fair 9 (21.95%)
Poor 2 (4.87%)
92% Substantial Improvement
in Pain
[Acta Orthopedica Hellenica, 2007]
www.shoulder.gr](https://image.slidesharecdn.com/vdmtfurgstkx7fomydpx-signature-69d9f1a3cb3f2649714837b93c1c3b7b41f9a67bbef005eecf911e10fcb33758-poli-170927100658/85/Rotator-cuff-2008-final-67-320.jpg)






























































![ROTATOR CUFF[4273].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/rotatorcuff4273-221222051719-751991ae-thumbnail.jpg?width=640&height=640&fit=bounds)















































