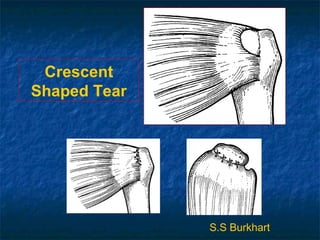
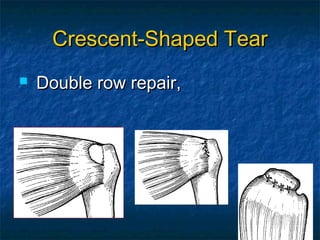
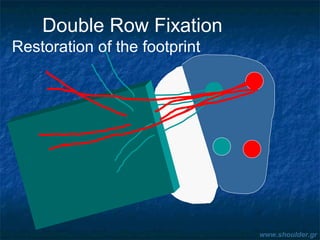
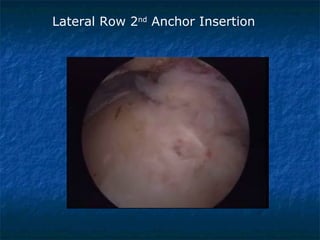
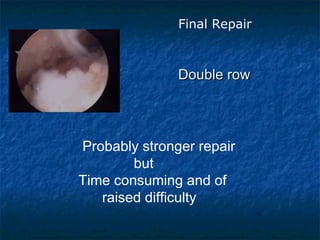
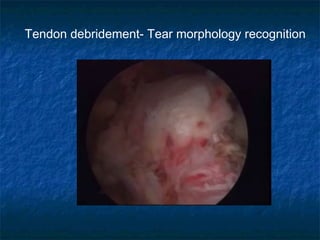
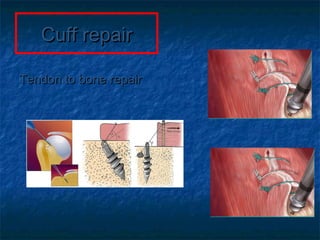
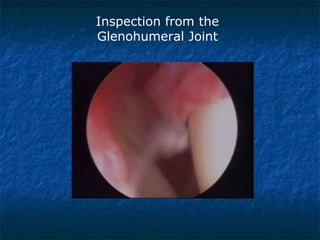
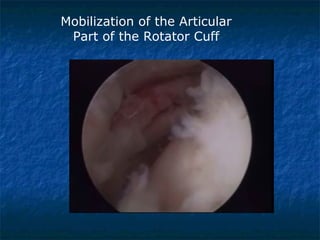
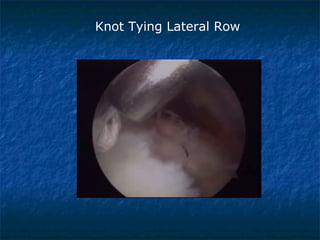
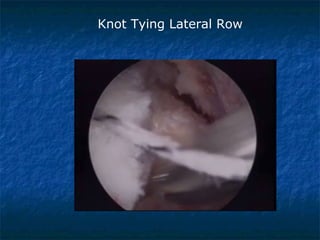
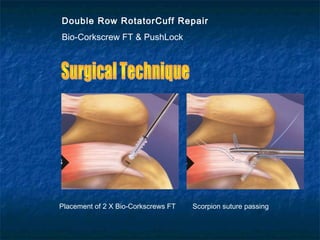
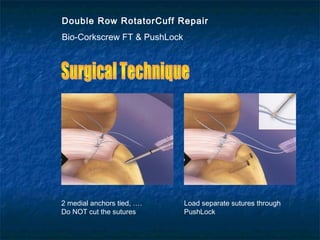
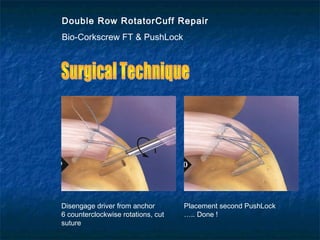
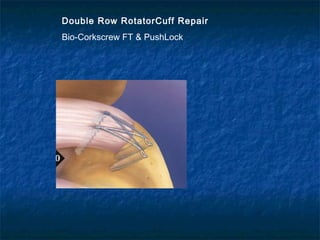
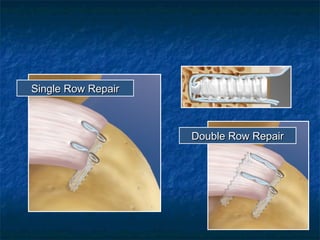
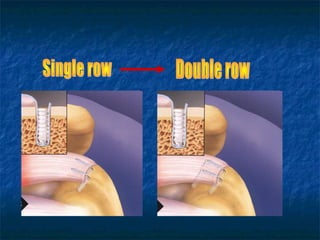
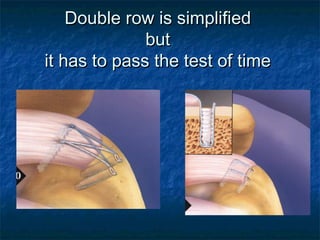
Massive rotator cuff tears present unique challenges for repair. The document discusses techniques for arthroscopic repair based on tear pattern, including releases to improve mobility. For crescent tears, a double row fixation is recommended. L-shaped and U-shaped tears are repaired with side-to-side sutures converging the margin. Massive contracted immobile tears may require interval slides. Outcomes are generally good, though strength deficits can remain. Proper patient selection considering fatty degeneration and mobility is important for success.











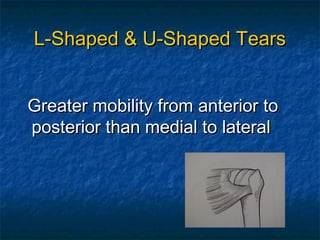
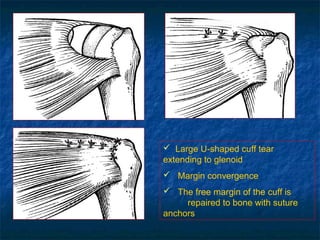
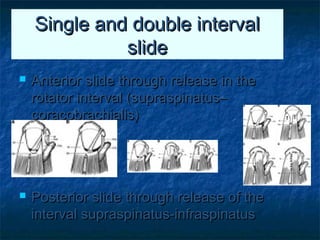
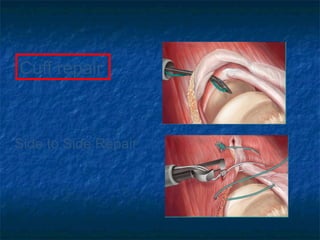
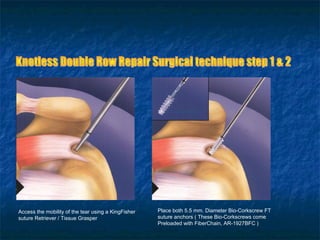
![L-Shaped & U-Shaped TearsL-Shaped & U-Shaped Tears
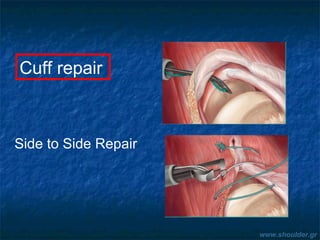
Side to side sutures from medial to lateralSide to side sutures from medial to lateral
Progressively converge the margin of theProgressively converge the margin of the
tear lateral to bone bedtear lateral to bone bed
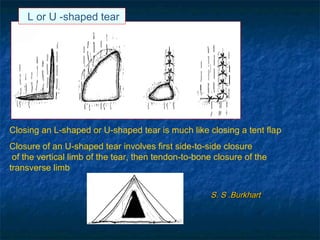
Closing 50% of a U-Shaped tear ->Closing 50% of a U-Shaped tear ->
reduces strain at converge margin by areduces strain at converge margin by a
factor of 6factor of 6
[[S. S .Burkhart]S. S .Burkhart]](https://image.slidesharecdn.com/sy3d2cqbtxsm0vuspt6b-signature-69d9f1a3cb3f2649714837b93c1c3b7b41f9a67bbef005eecf911e10fcb33758-poli-170927100657/85/Massive-rot-cuf-26-320.jpg)

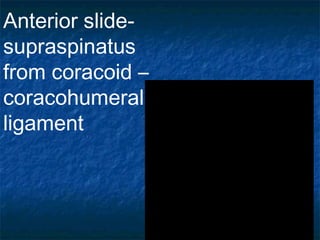
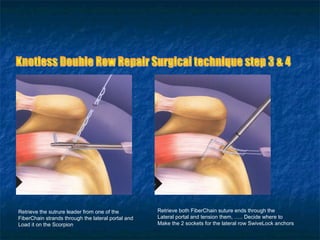
![Massive Contracted ImmobileMassive Contracted Immobile
TearsTears
No mobility from medial to lateral or fromNo mobility from medial to lateral or from
anterior to posterioranterior to posterior
Subcategories:Subcategories:
Massive Contracted Longitudinal TearsMassive Contracted Longitudinal Tears
Massive Contracted Crescent TearsMassive Contracted Crescent Tears
Represent 9.6% of massive tearsRepresent 9.6% of massive tears
[[S.Burkhart]S.Burkhart]](https://image.slidesharecdn.com/sy3d2cqbtxsm0vuspt6b-signature-69d9f1a3cb3f2649714837b93c1c3b7b41f9a67bbef005eecf911e10fcb33758-poli-170927100657/85/Massive-rot-cuf-32-320.jpg)


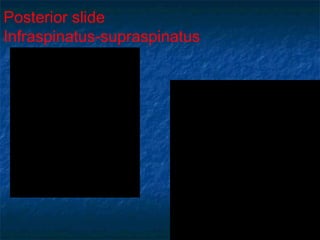


![Results for massive tearsResults for massive tears
95% Good to Excellent Results95% Good to Excellent Results
independent to tear sizeindependent to tear size [Burkhart, 2001][Burkhart, 2001]
With interval slideWith interval slide
Improve UCLA score (10->28.3)Improve UCLA score (10->28.3)
Improve Active ROM, StrengthImprove Active ROM, Strength
[Burkhart, 2004][Burkhart, 2004]
Graft Jacket RepairGraft Jacket Repair
Improve UCLA score (18->32Improve UCLA score (18->32))
[Snyder, 2008][Snyder, 2008]](https://image.slidesharecdn.com/sy3d2cqbtxsm0vuspt6b-signature-69d9f1a3cb3f2649714837b93c1c3b7b41f9a67bbef005eecf911e10fcb33758-poli-170927100657/85/Massive-rot-cuf-49-320.jpg)
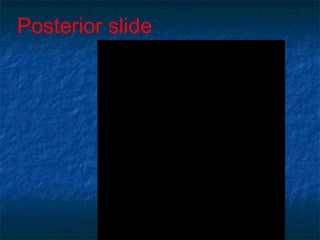
![What to do???What to do???
Patients with grade 3 or 4 fatty degenerationPatients with grade 3 or 4 fatty degeneration
DO NOTDO NOT improve with rot cuff repairimprove with rot cuff repair
[Goutallier][Goutallier]
Vs.Vs.
Patients with grade 3 or 4 fatty degenerationPatients with grade 3 or 4 fatty degeneration
improved significant at 86% of cases afterimproved significant at 86% of cases after
arthroscopic repairarthroscopic repair
[Burkhart][Burkhart]](https://image.slidesharecdn.com/sy3d2cqbtxsm0vuspt6b-signature-69d9f1a3cb3f2649714837b93c1c3b7b41f9a67bbef005eecf911e10fcb33758-poli-170927100657/85/Massive-rot-cuf-51-320.jpg)



























































![ROTATOR CUFF[4273].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/rotatorcuff4273-221222051719-751991ae-thumbnail.jpg?width=640&height=640&fit=bounds)





















![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)


















