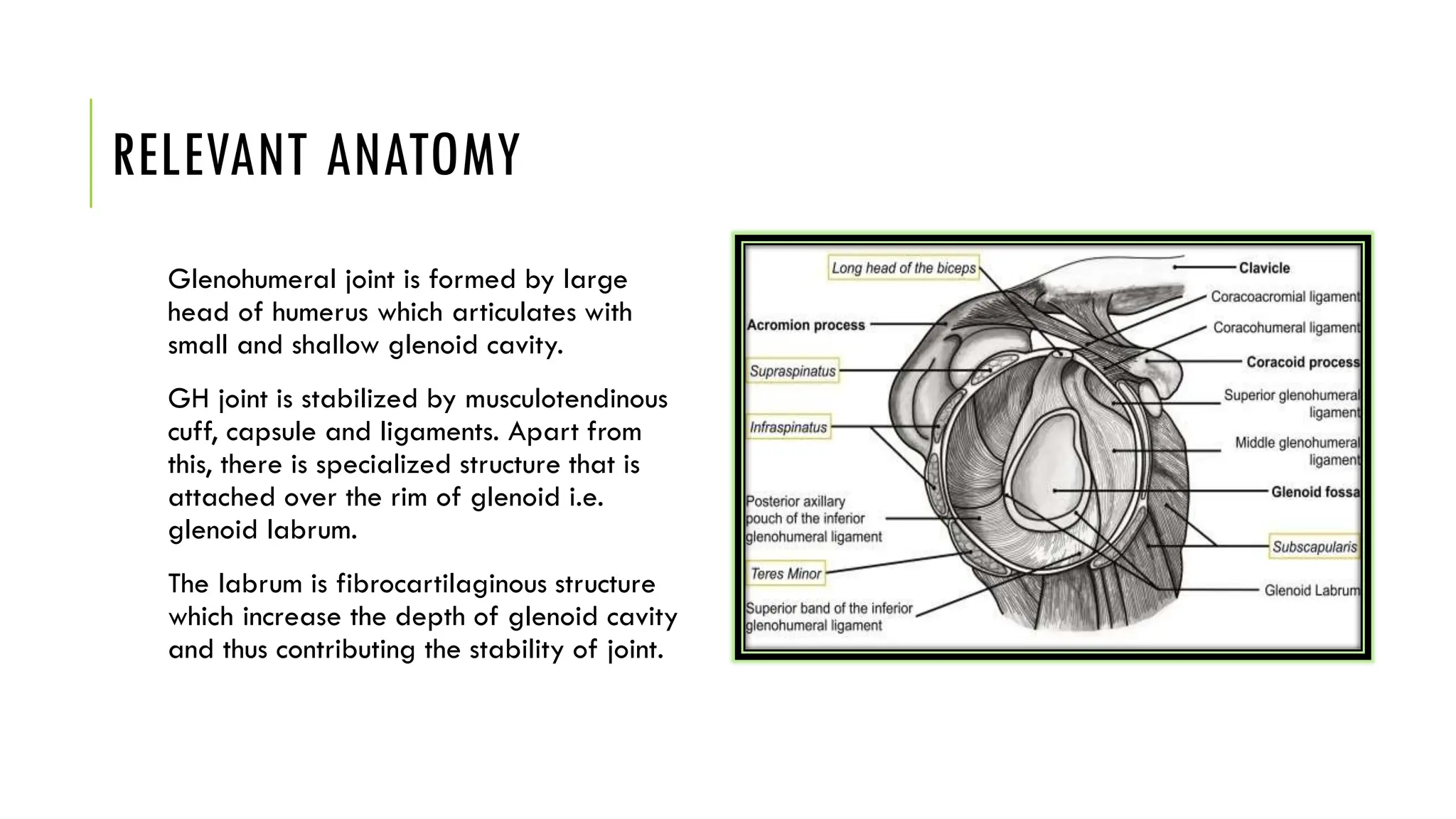
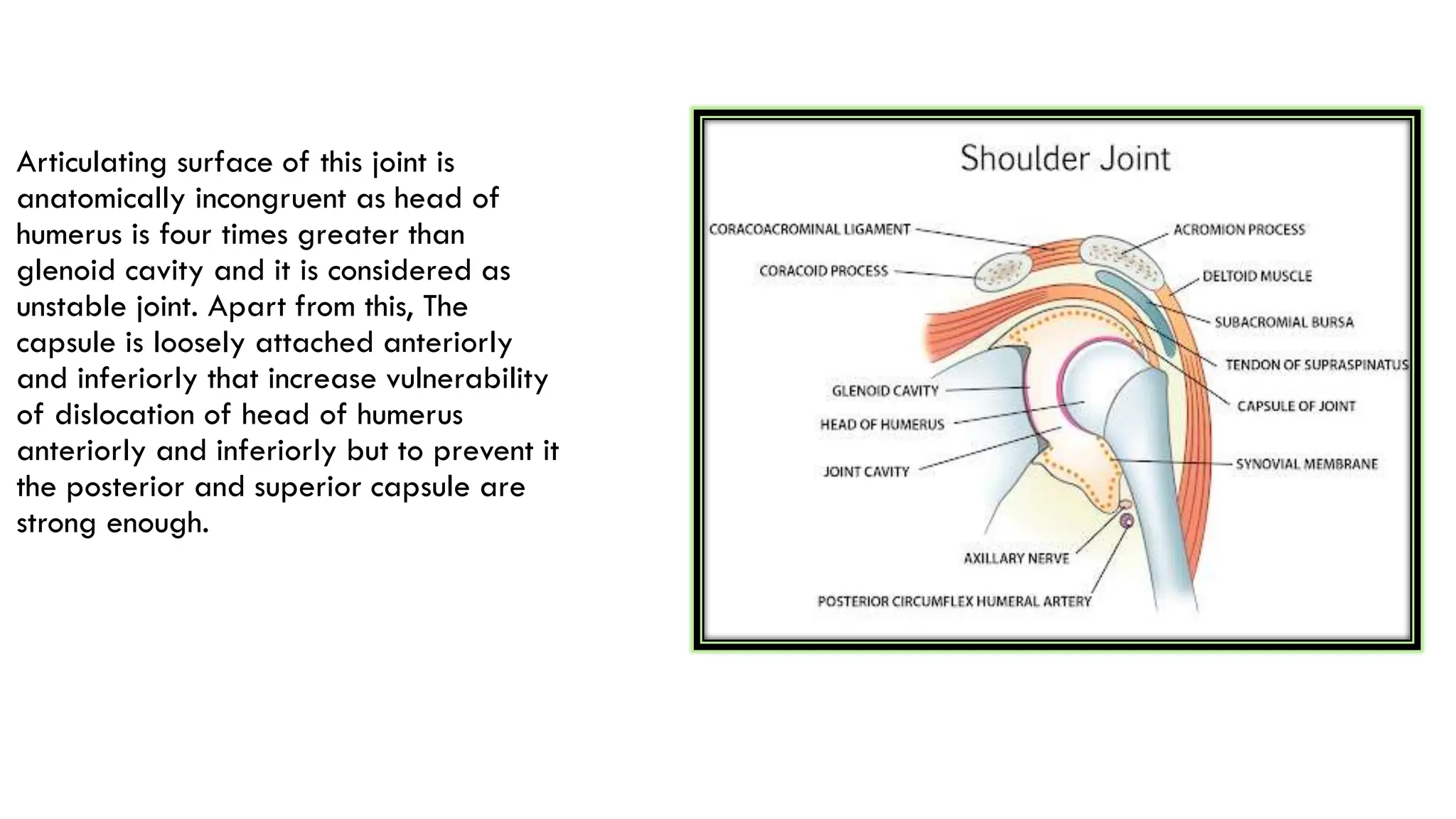
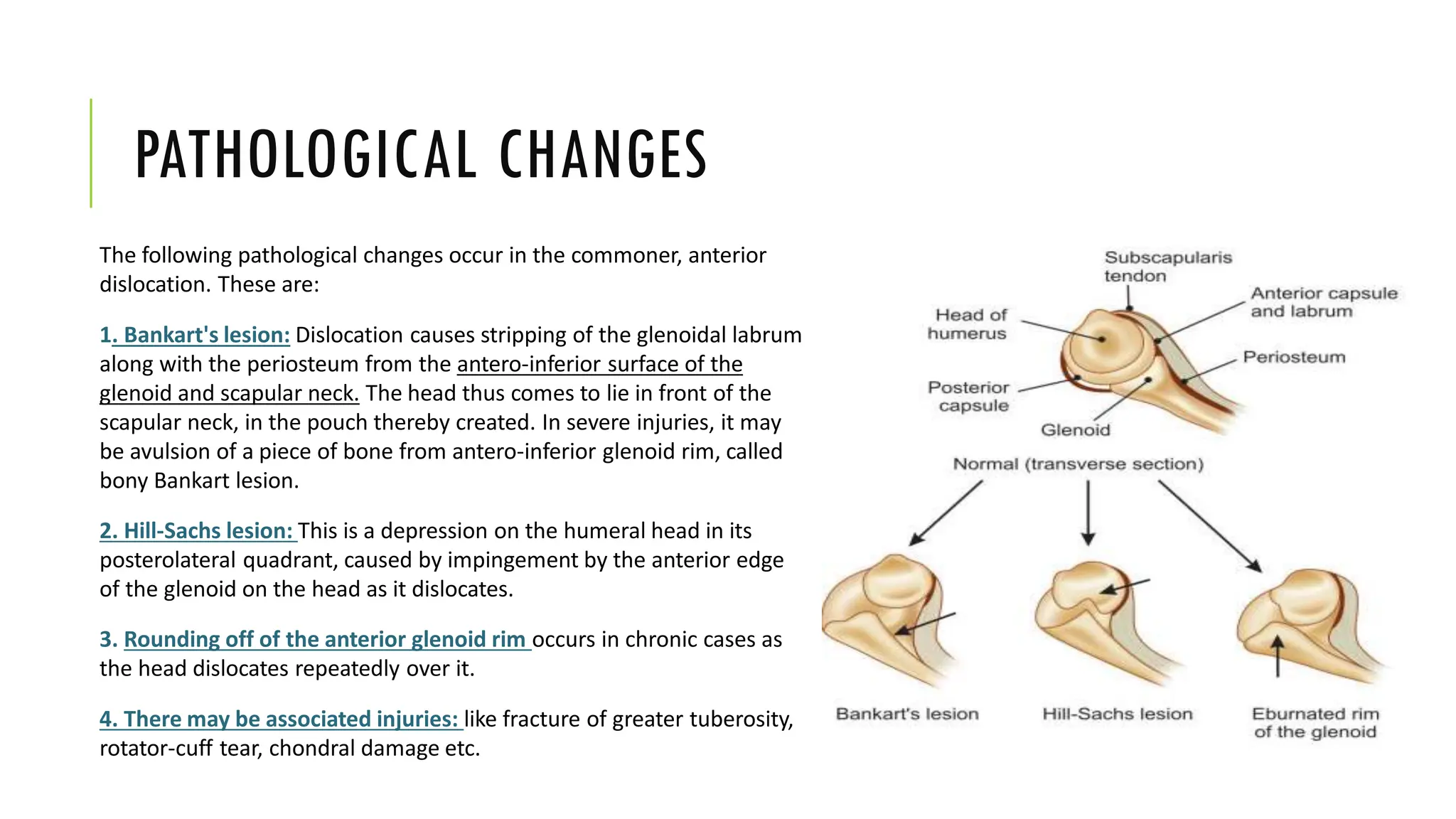
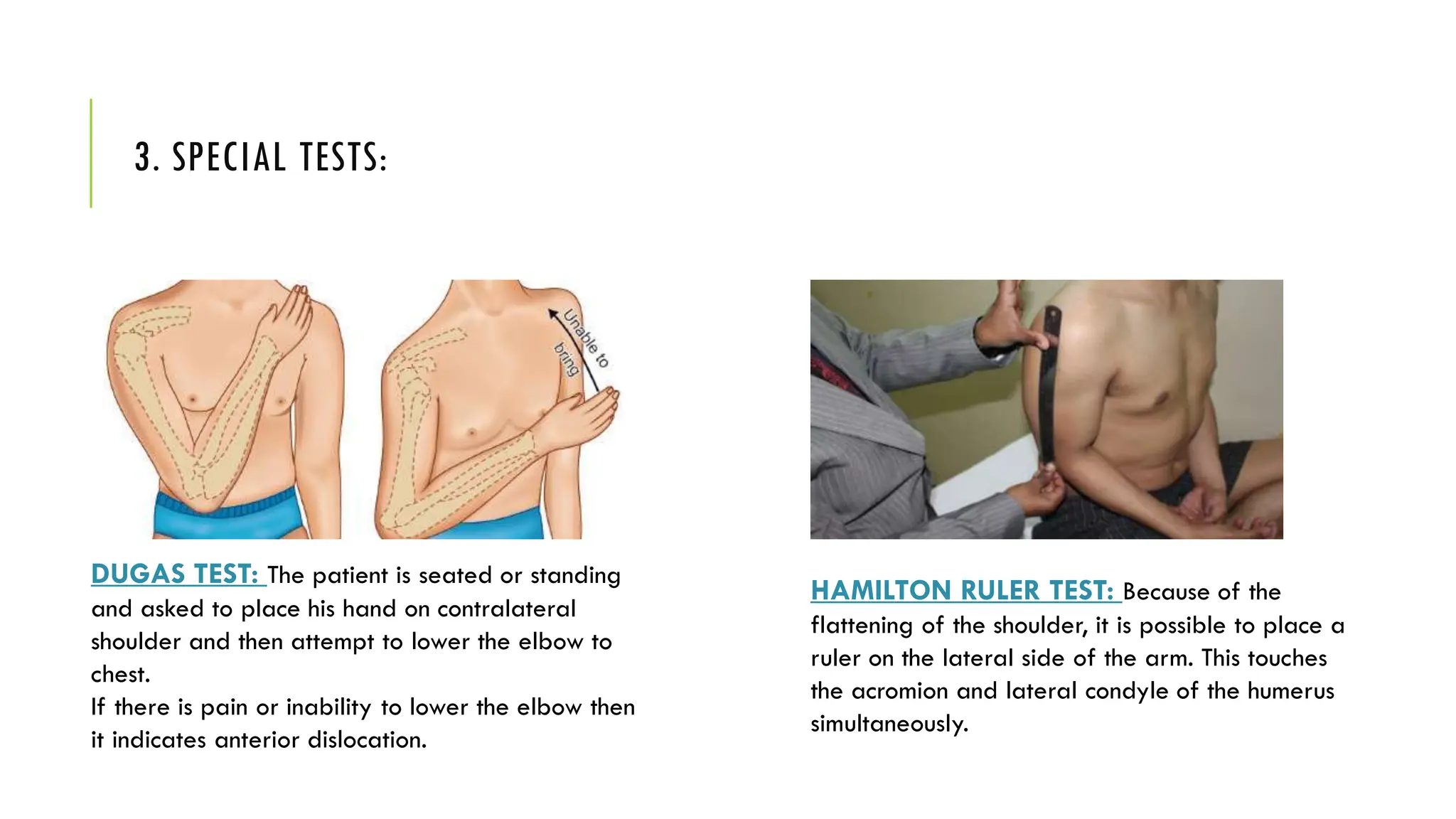
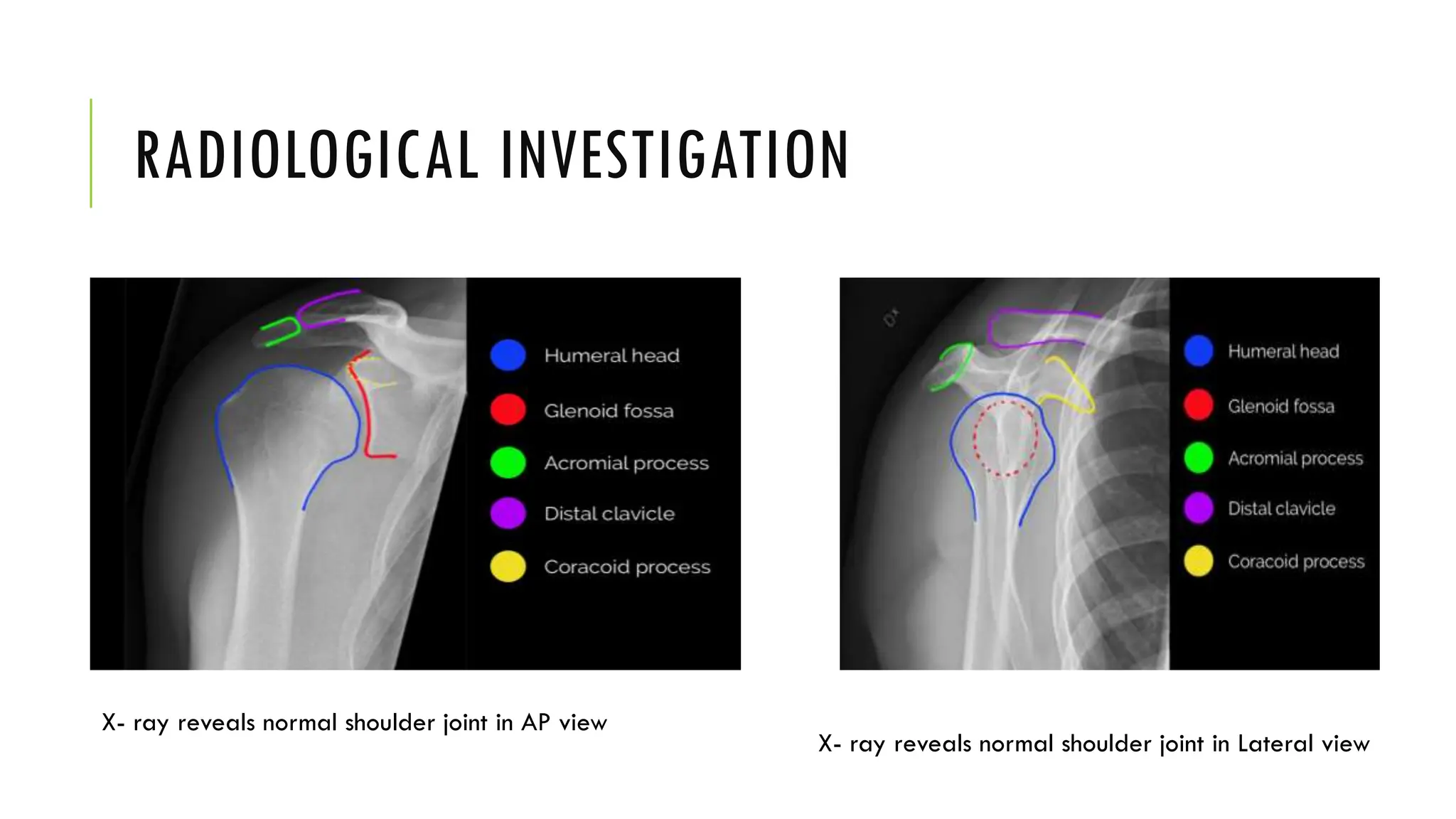
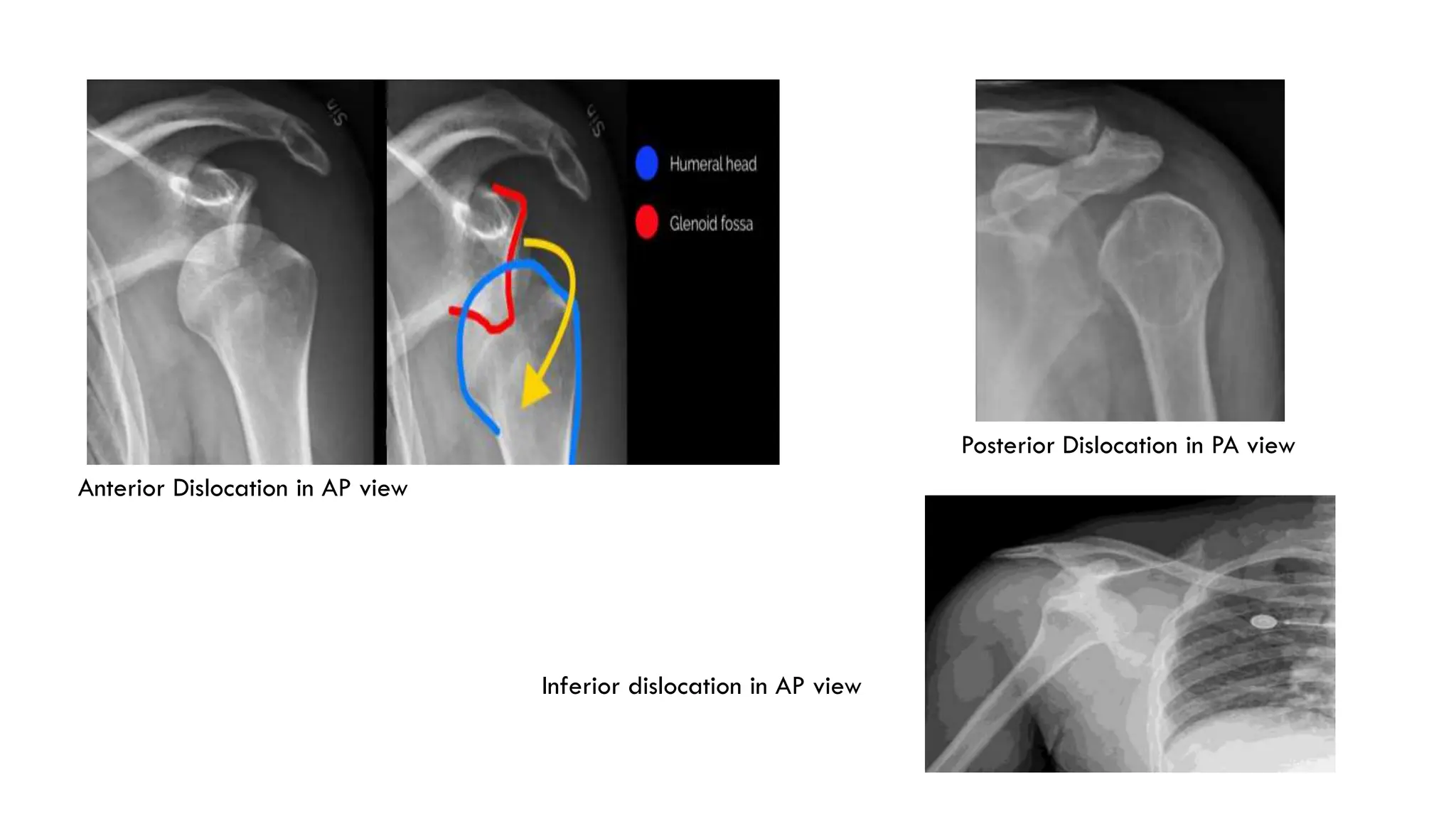
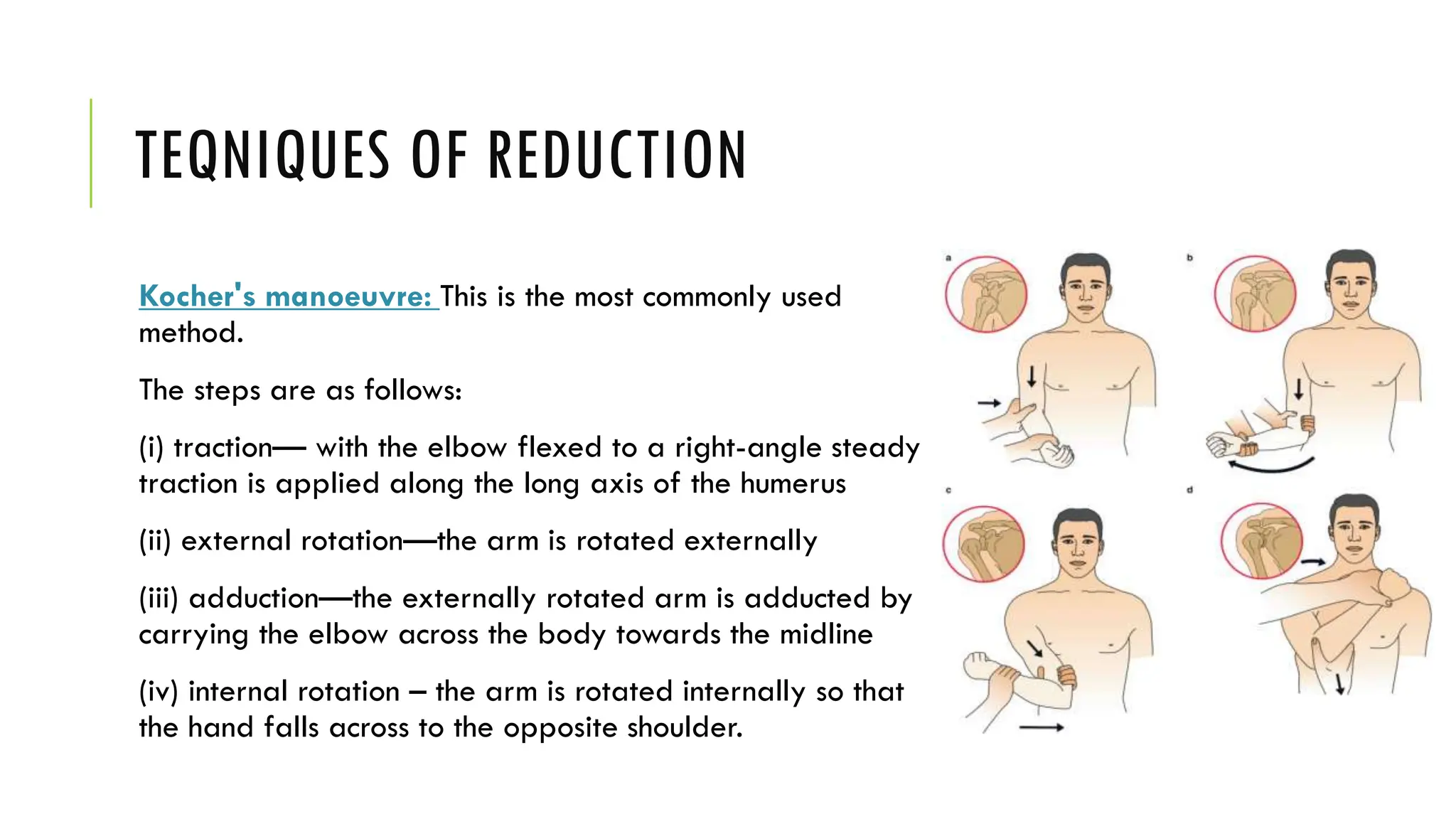
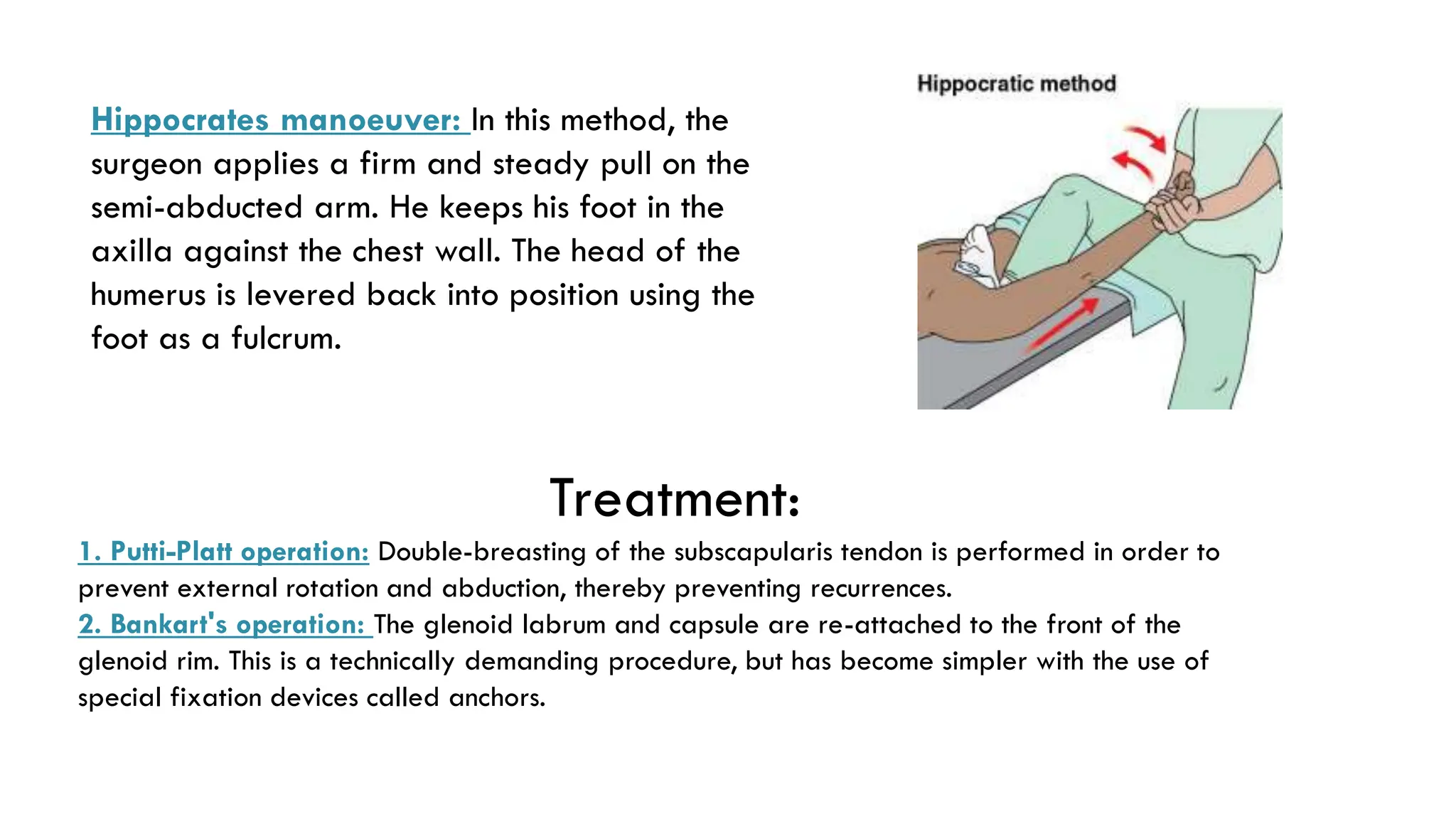
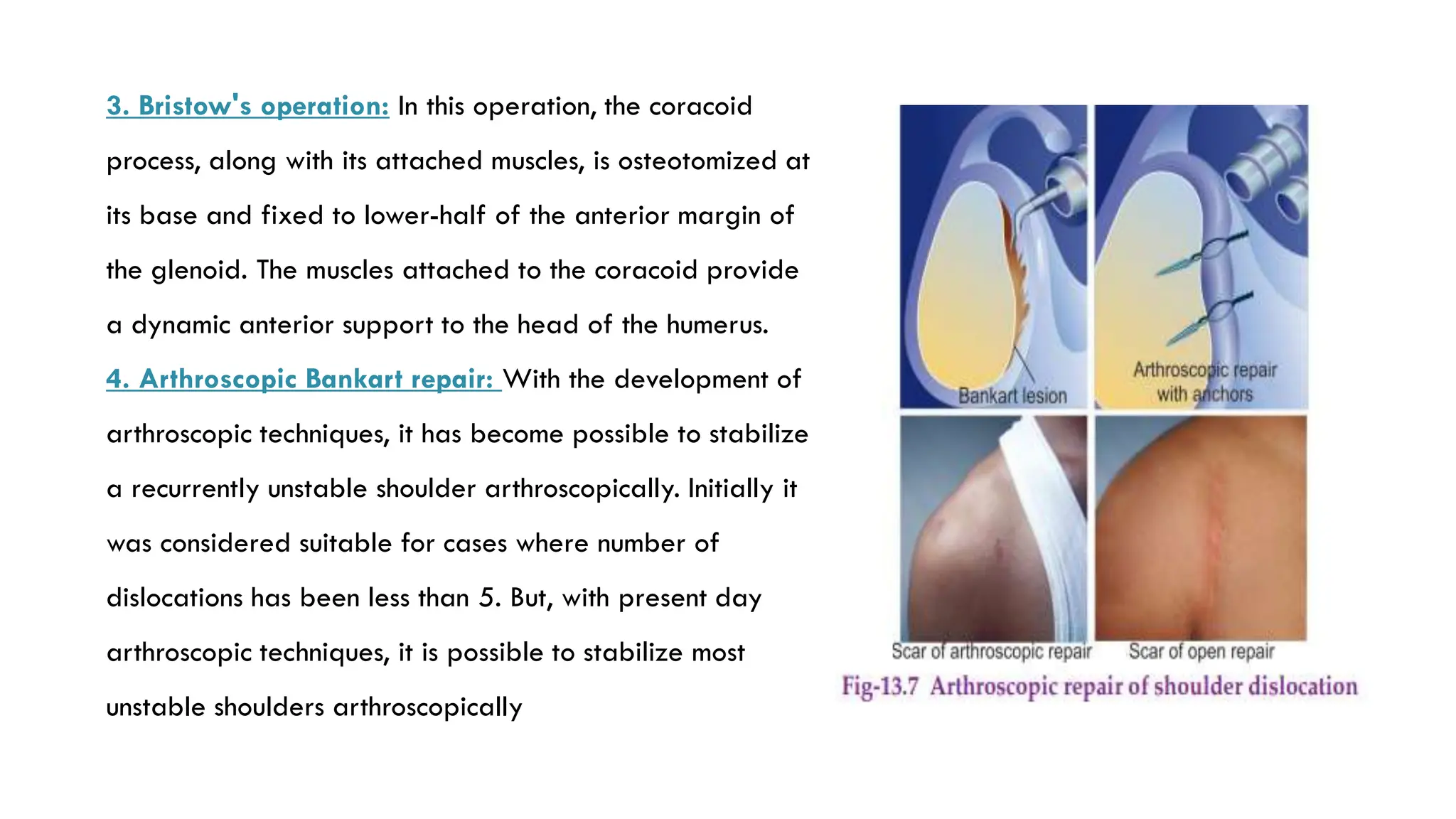
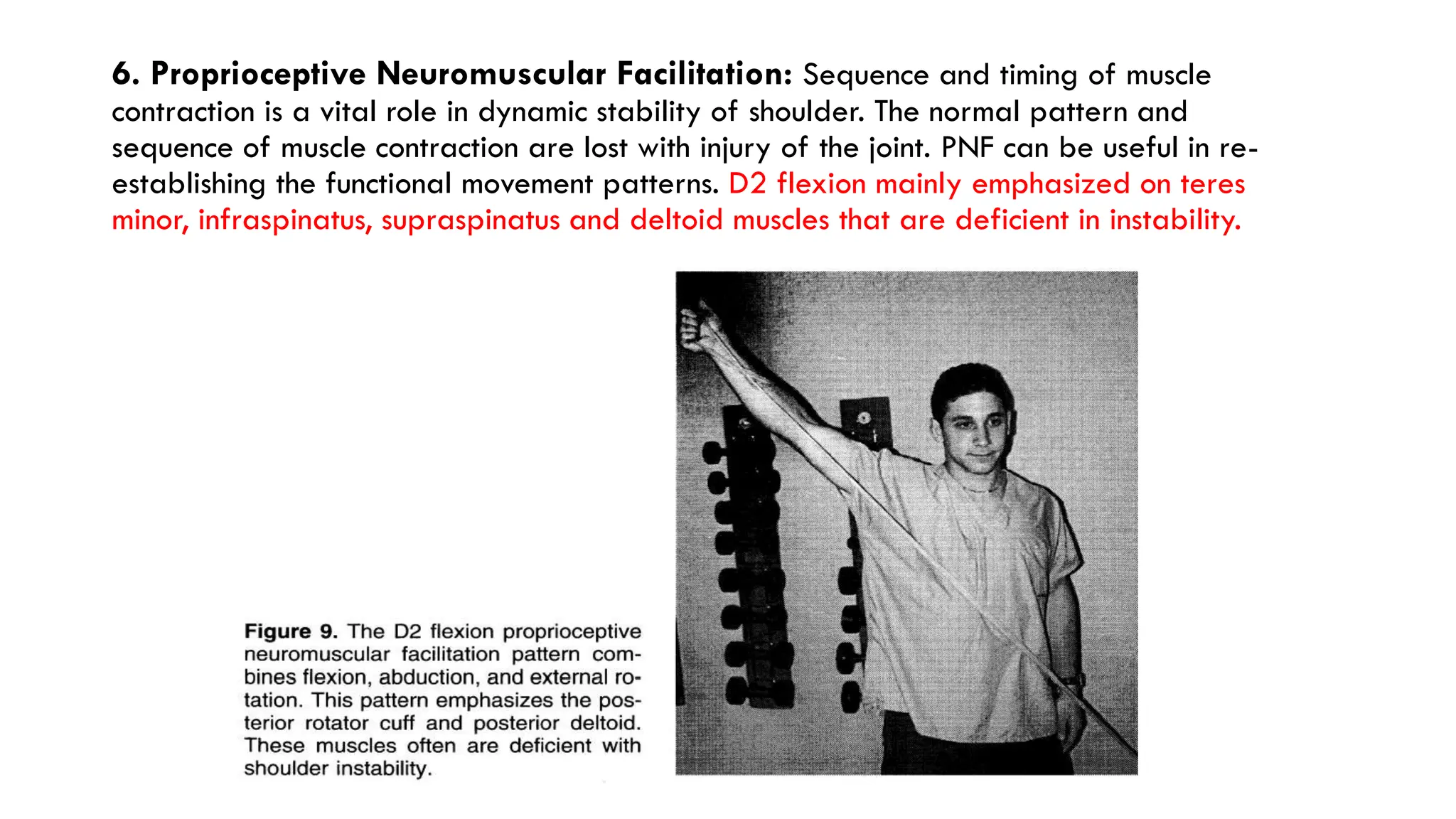
The document discusses shoulder dislocation, focusing on relevant anatomy, mechanisms, classification, pathological changes, diagnosis, techniques of reduction, and management strategies including surgical and rehabilitation approaches. Anterior dislocations are the most common, with specific subtypes and associated injuries detailed, along with diagnostic methods and radiological evaluations. Post-surgical rehabilitation protocols emphasize cryotherapy, activity restrictions, isometric and range of motion exercises, scapulothoracic retraining, and proprioceptive neuromuscular facilitation for optimal recovery.