Downloaded 191 times
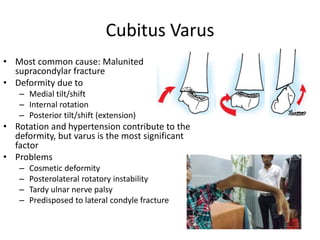



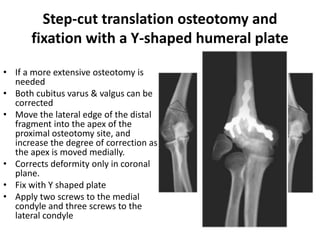
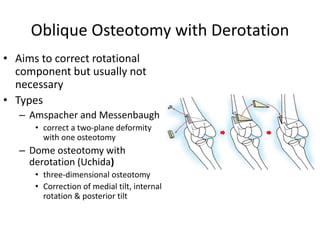


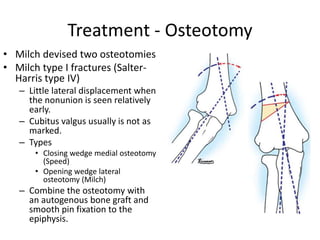

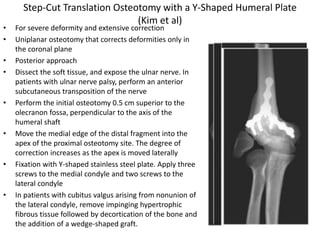


Osteotomy around the elbow is commonly performed to correct cubitus varus and cubitus valgus deformities. For cubitus varus, the most common cause is a malunited supracondylar fracture. Surgical options include lateral closing wedge osteotomy, oblique osteotomy with derotation, and medial opening wedge osteotomy with bone grafting. For cubitus valgus, causes include nonunion of a lateral condyle fracture. Surgical options are a closing wedge medial osteotomy or opening wedge lateral osteotomy. Complications of elbow osteotomy can include stiffness, persistent deformity, myositis ossificans, loss of fixation, and neurovascular injury.



































































