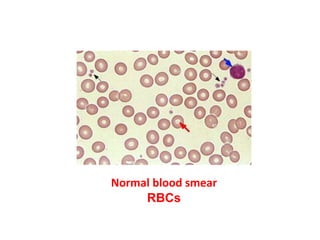
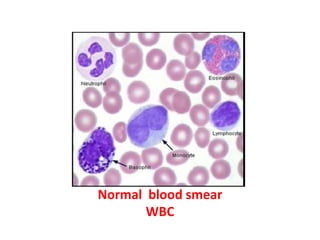
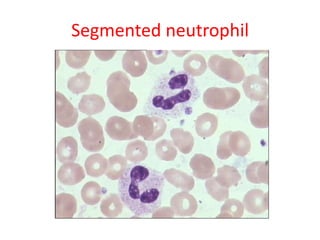
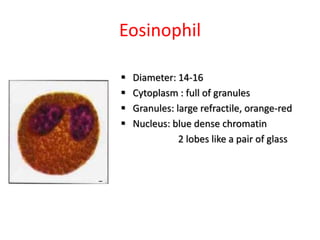
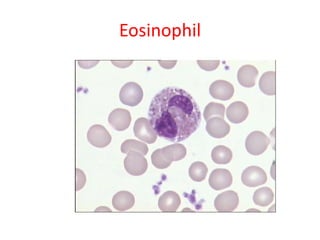
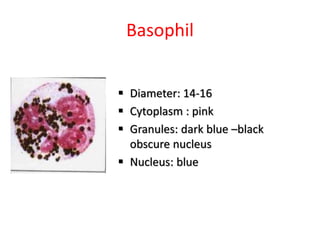

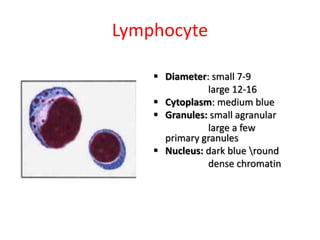
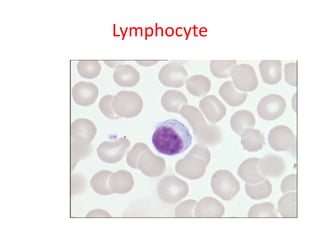
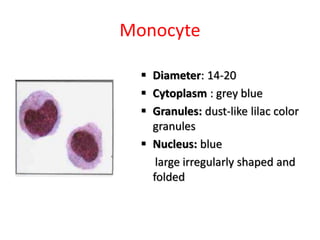
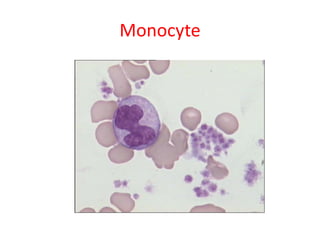
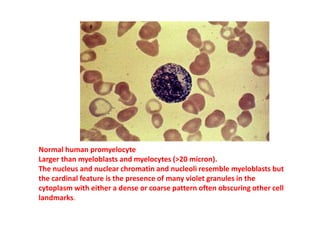
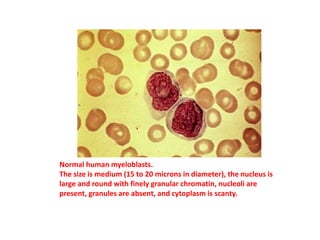
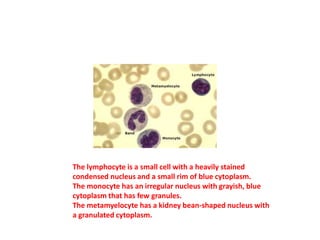
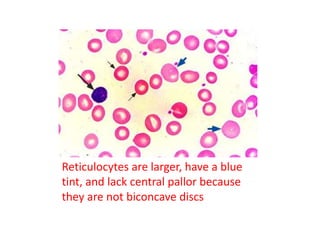
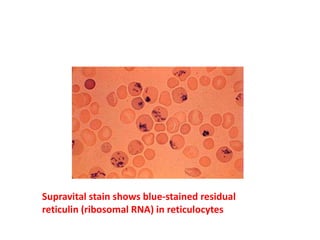
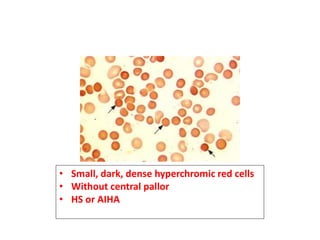
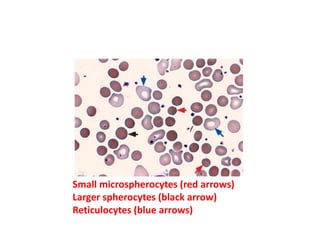
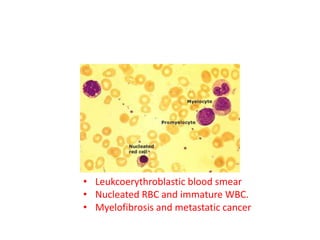
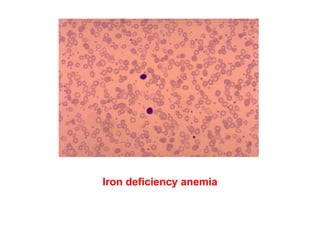
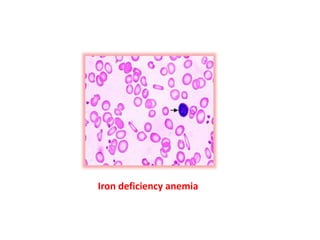
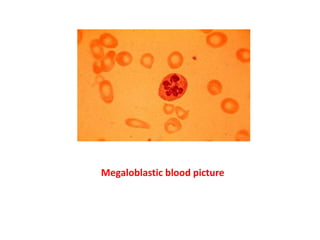
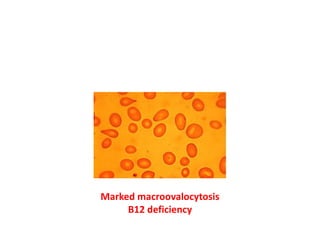
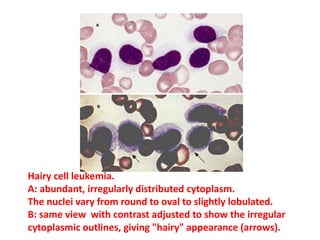
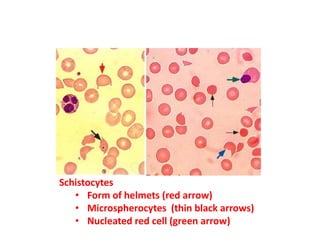
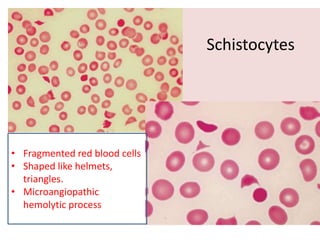
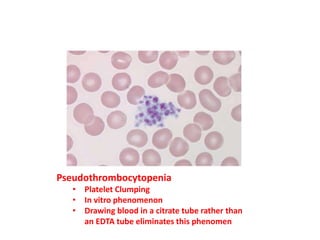
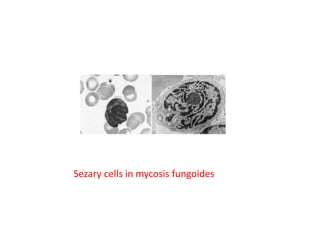
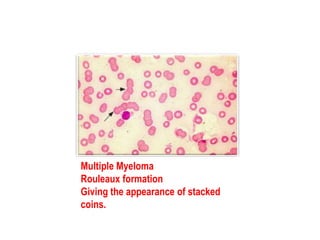
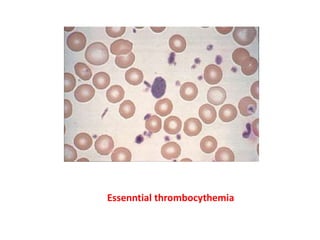
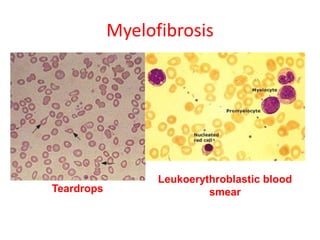
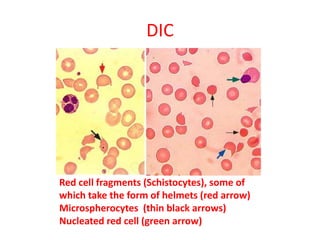
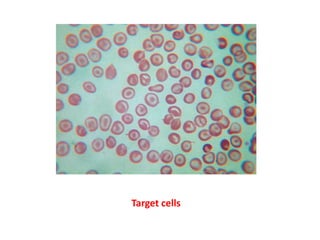
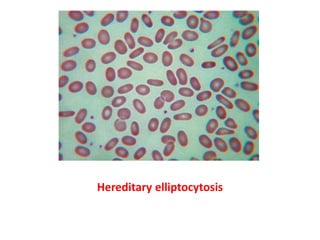
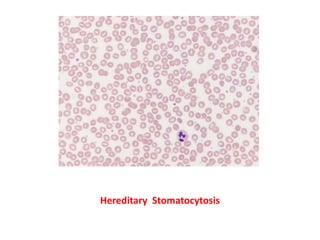

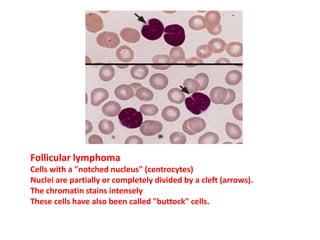
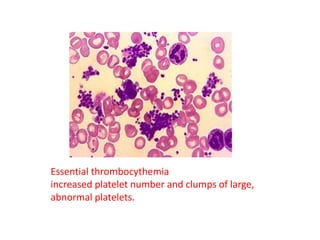
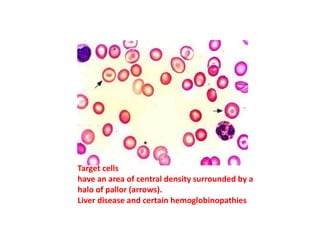
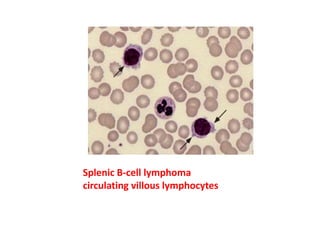


The document provides a detailed evaluation of peripheral blood smear findings, highlighting various blood cell types such as red blood cells, white blood cells, and their characteristics in normal and pathological conditions. It discusses specific abnormalities associated with anemia, leukemia, infections, and other hematological disorders, illustrated with descriptions of cell morphology and features. Additionally, it mentions diseases like myelofibrosis, sickle cell anemia, and lead poisoning, including relevant diagnostic features observed under a microscope.



































































