

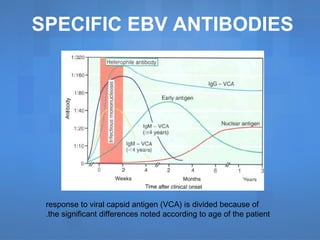


Infectious mononucleosis, primarily caused by the Epstein-Barr virus (EBV), presents with symptoms such as fatigue, fever, and lymphadenopathy. EBV infects over 95% of the global population, leading to lifelong latent infections and is associated with several malignancies, particularly in immunocompromised individuals. Diagnosis involves clinical symptoms and laboratory tests showing atypical lymphocytosis, with treatment primarily focused on supportive care and corticosteroids for complications.






![Epstein barr virus [autosaved]](https://cdn.slidesharecdn.com/ss_thumbnails/epsteinbarrvirusautosaved-211025044258-thumbnail.jpg?width=640&height=640&fit=bounds)
















































































