


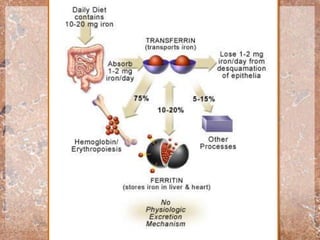




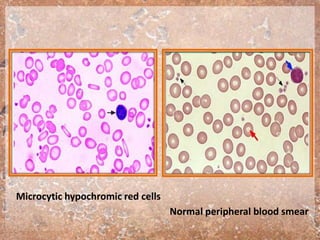
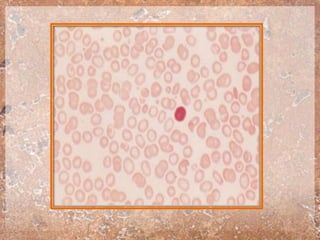





Iron deficiency is the most common nutritional deficiency affecting a significant portion of the global population, particularly preschool-aged children and women. Common causes include insufficient dietary intake, gastrointestinal malabsorption, and various perinatal factors, leading to clinical manifestations such as microcytic, hypochromic anemia and related developmental issues. Treatment primarily involves oral iron therapy alongside dietary modifications to prevent long-term deficiency effects.











































































































