The document discusses blood film examination and abnormalities seen in red blood cells. Key points include:
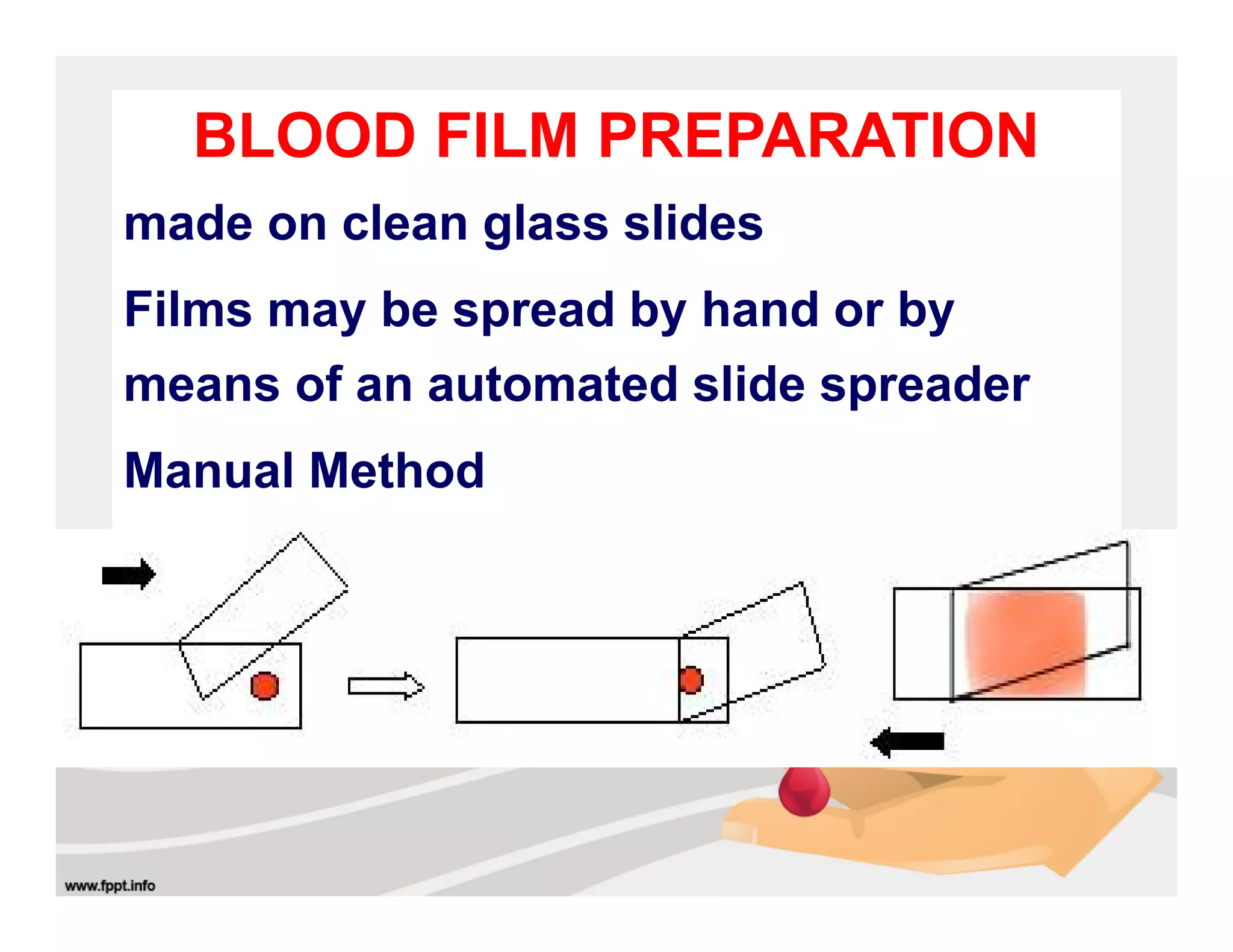
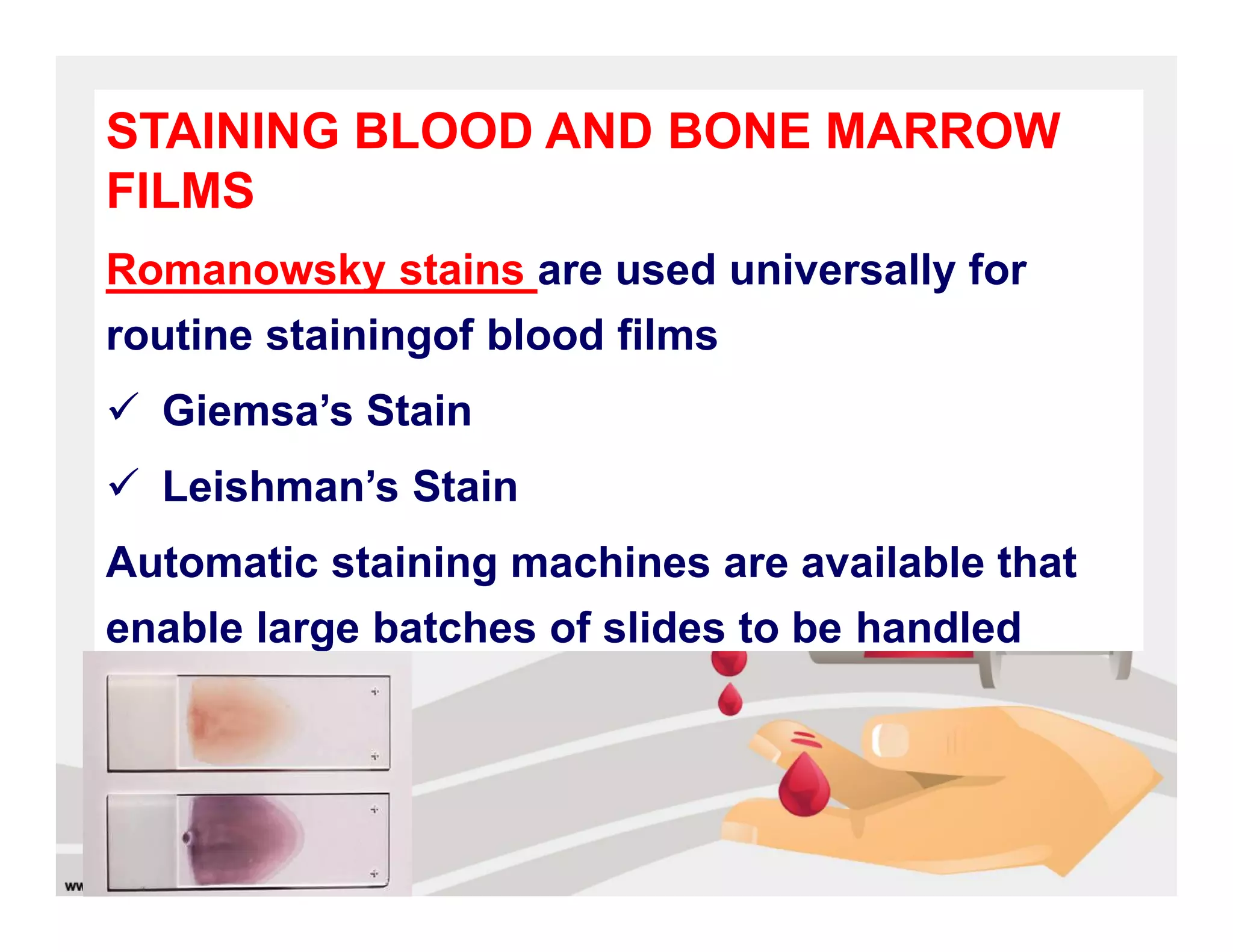
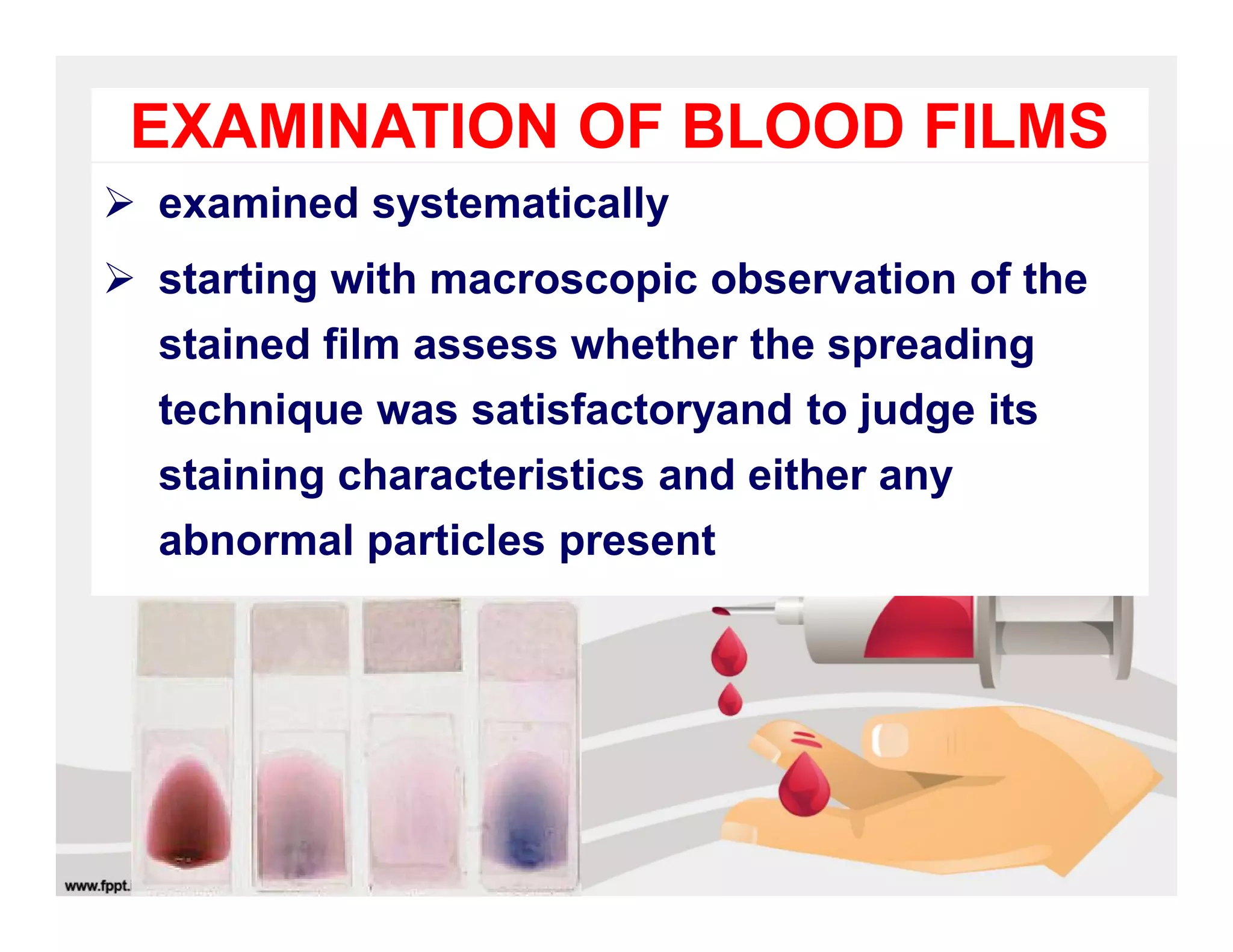
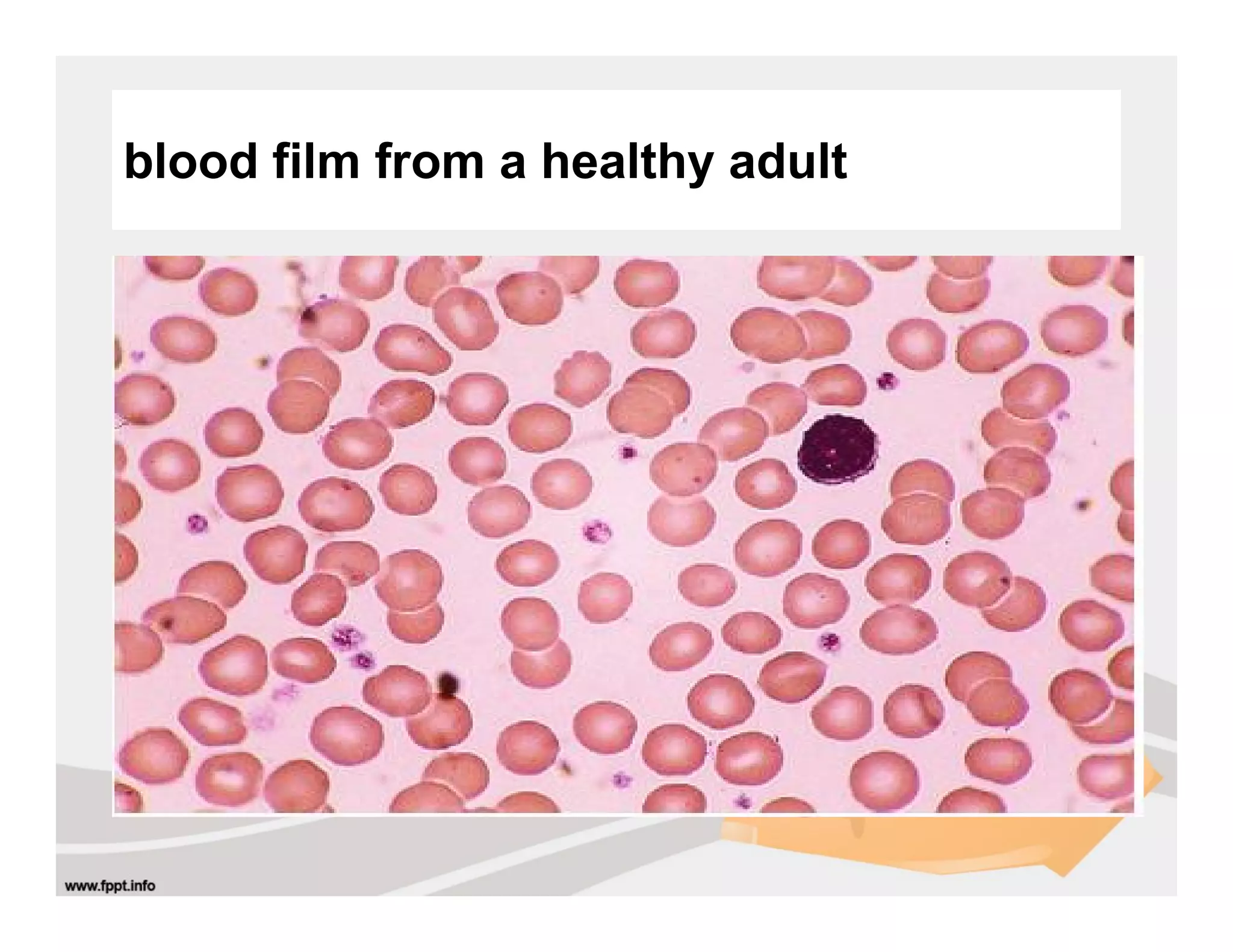
Blood films are prepared manually or automatically and stained using Romanowsky stains like Giemsa or Leishman's. Films are examined under low then high power microscopy to assess cell morphology and identify abnormalities.
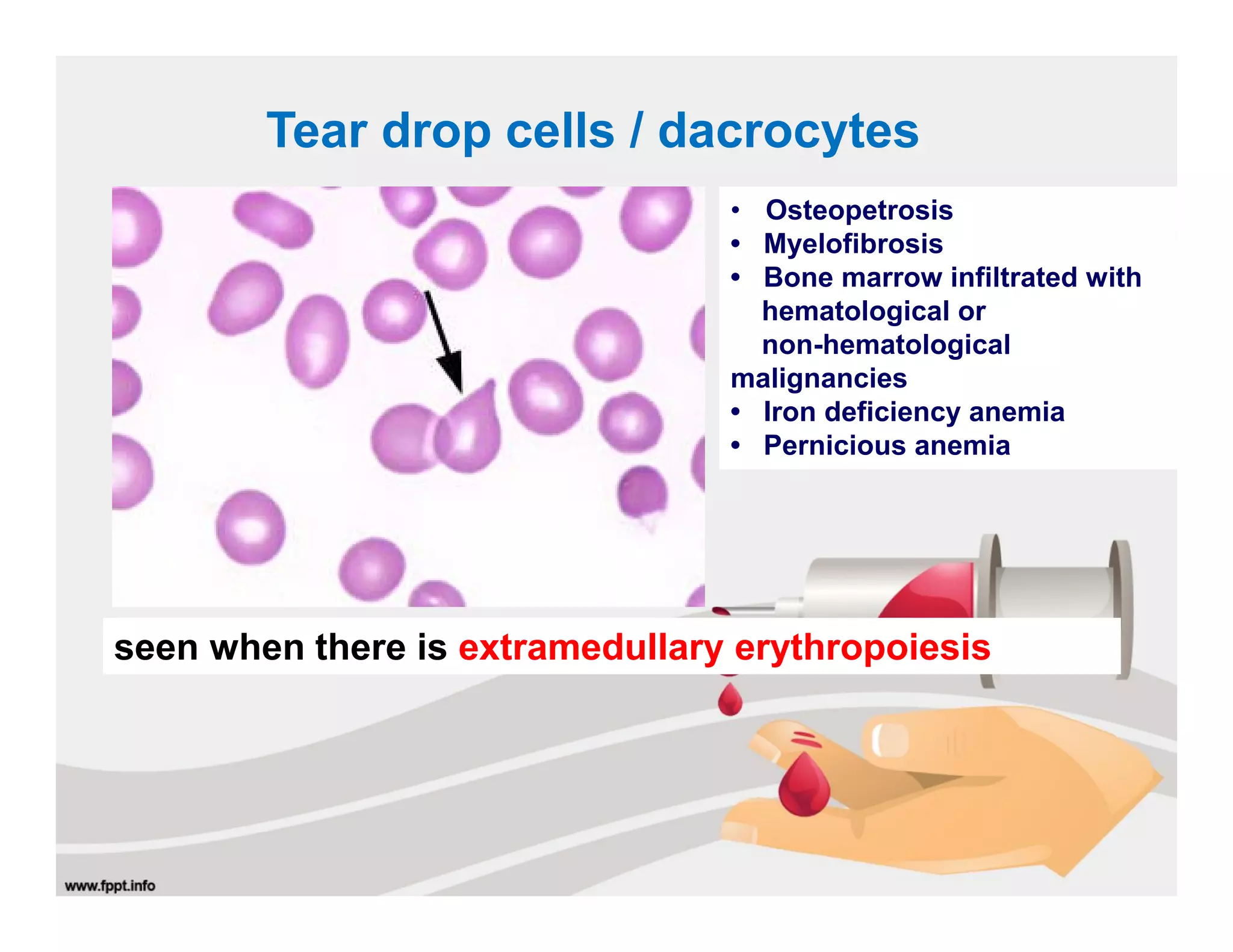
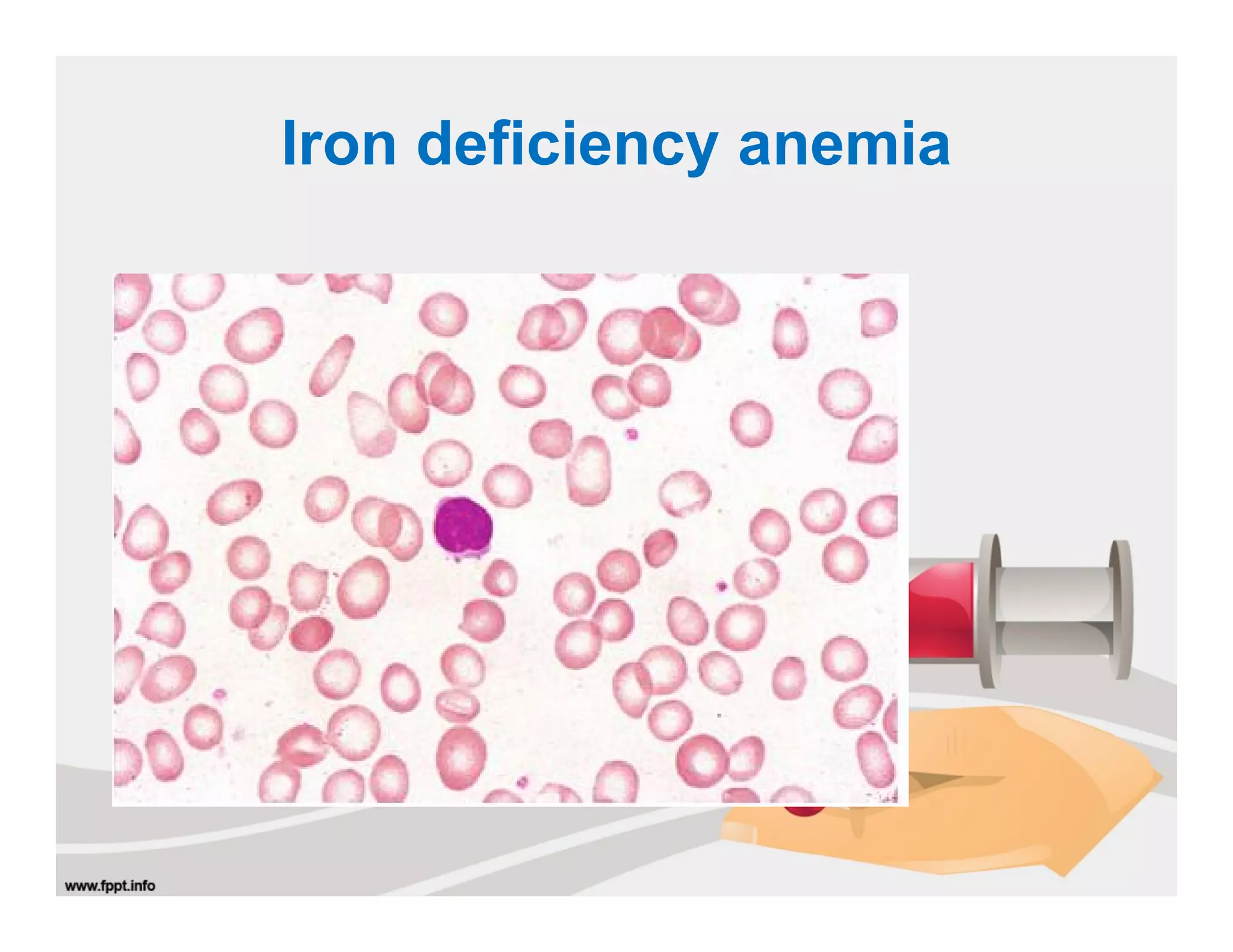
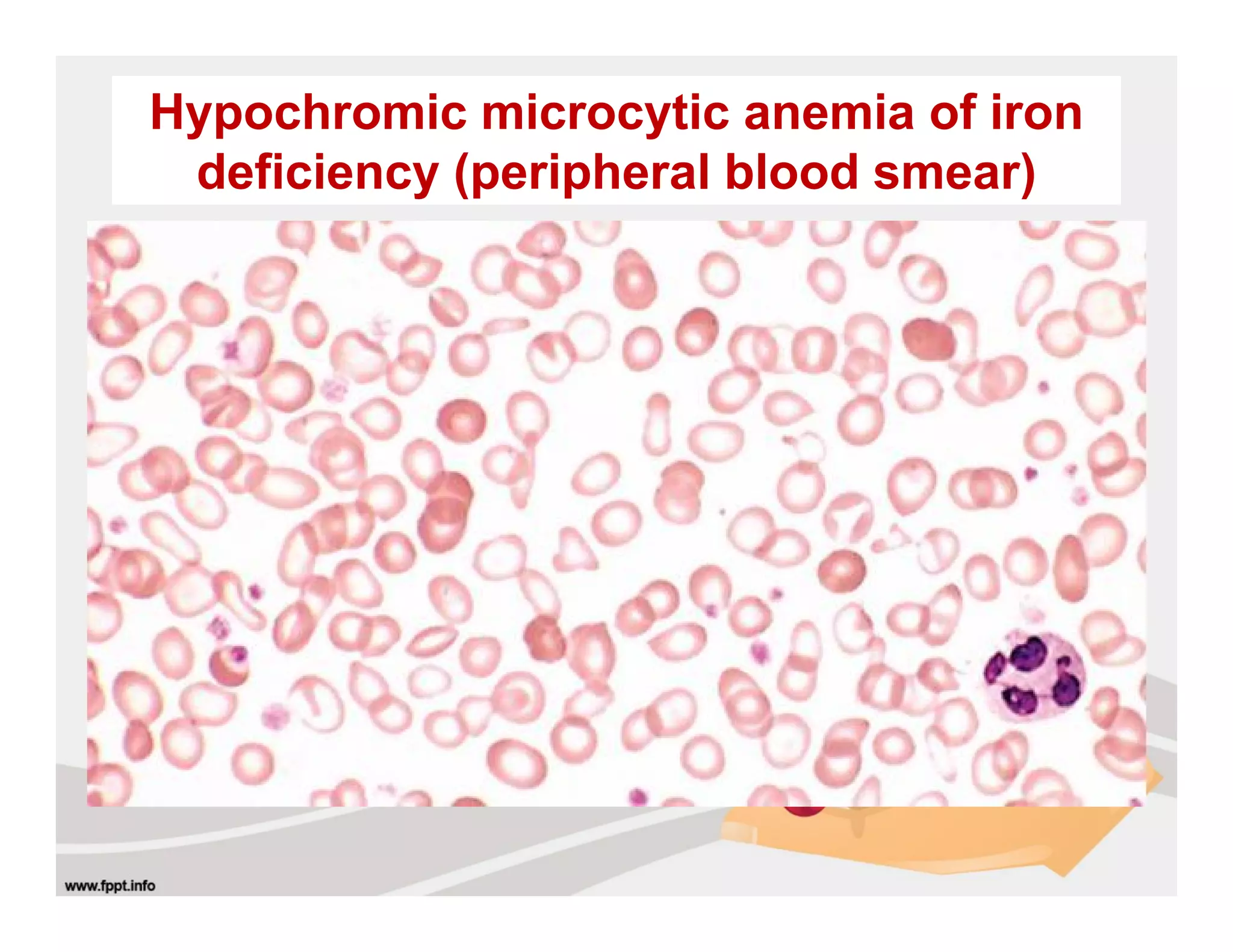
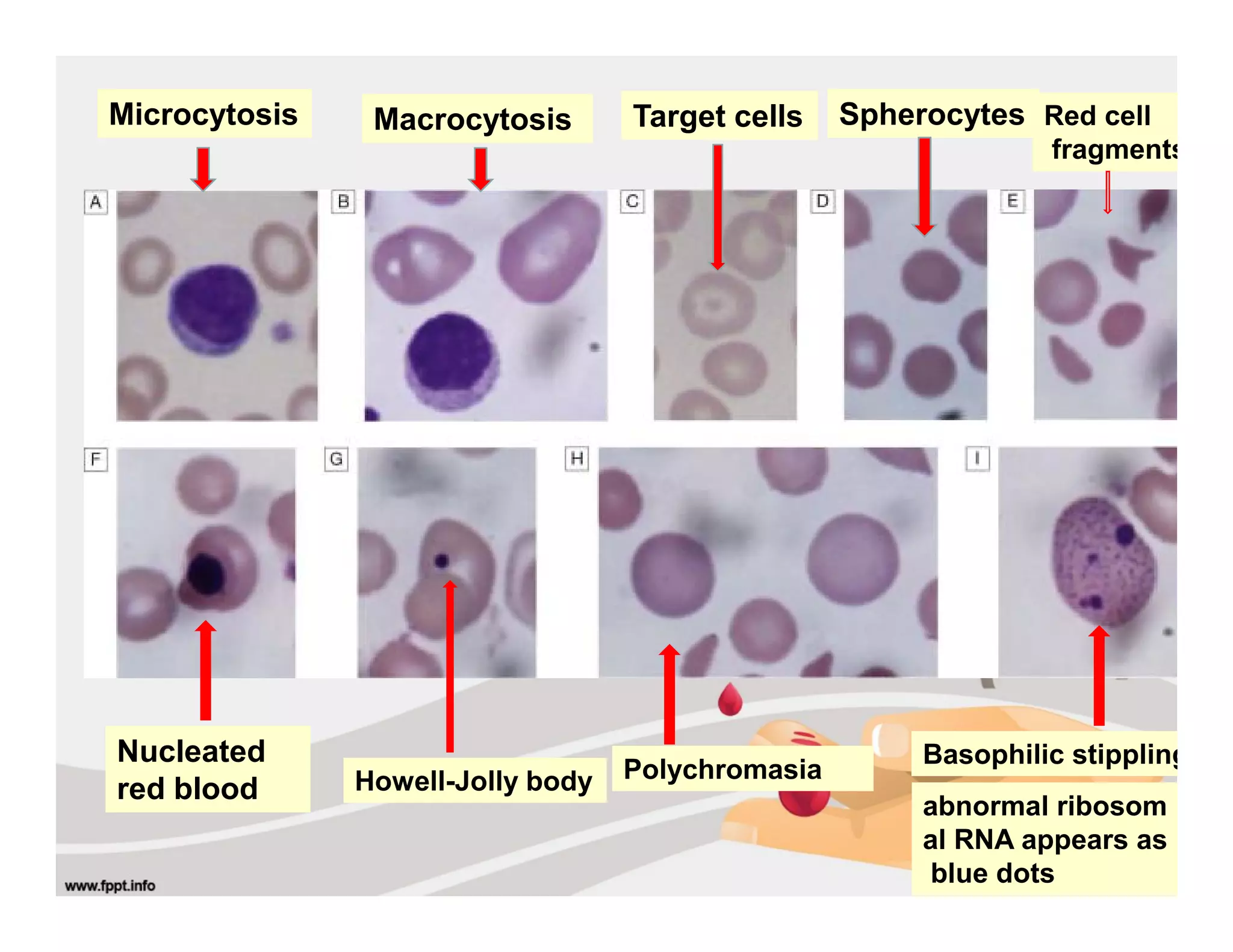
Abnormal red blood cell morphology seen in various anemias includes microcytosis in iron deficiency, macrocytosis in megaloblastic anemia, poikilocytosis in thalassemia, and hypochromia in iron deficiency. Specific abnormalities include target cells, sickle cells, spherocytes, and nucleated red blood cells. The differential diagnosis is considered based on the