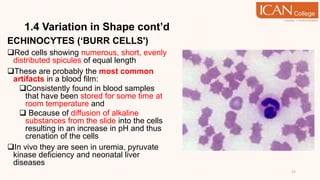
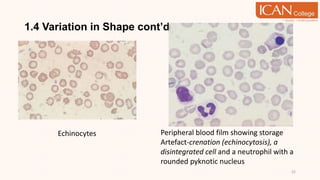
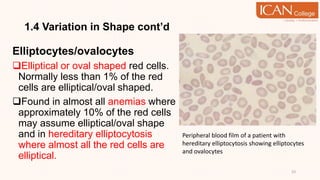
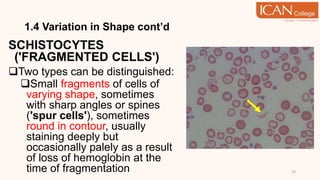
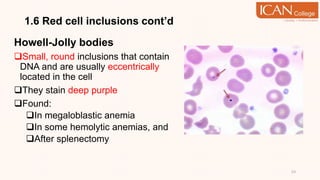
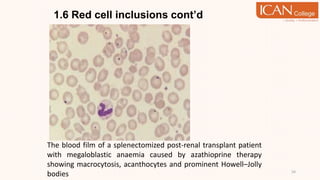
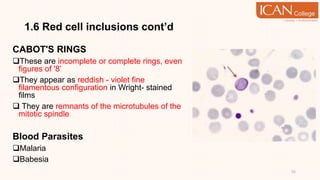
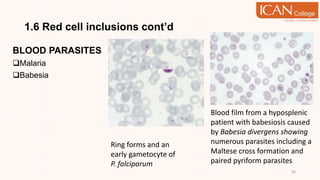
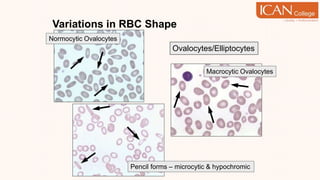
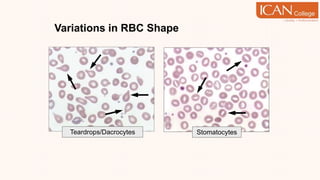
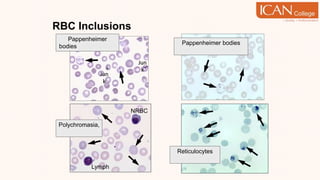
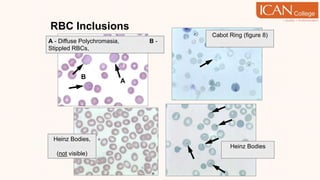
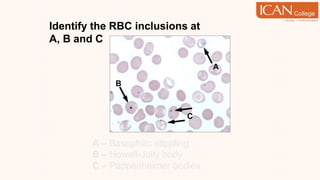
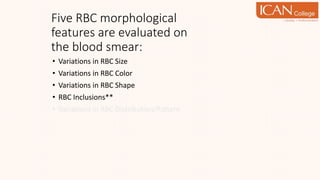
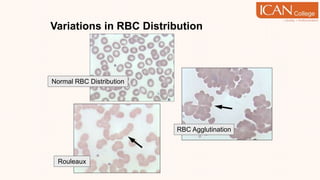
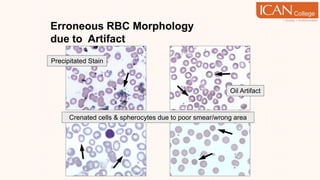
The document provides an in-depth study of red cell morphology, emphasizing the assessment of both normal and abnormal erythrocyte forms using stained blood films. It discusses various morphological features such as variations in size, shape, color, and specific inclusions in red blood cells, as well as their relevance in diagnosing hematologic disorders. Additionally, it covers abnormalities in red cell hemoglobinization and the grading system used for evaluating changes in erythrocyte morphology.











































































![Cells and Organs of immune system [Autosaved].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/cellsandorgansofimmunesystemautosaved-260123152717-ea0cb261-thumbnail.jpg?width=640&height=640&fit=bounds)













