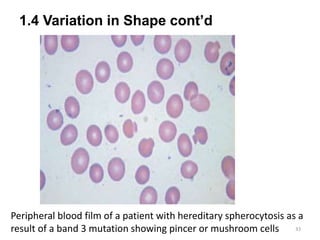
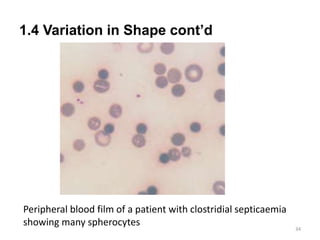
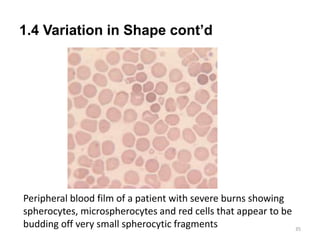
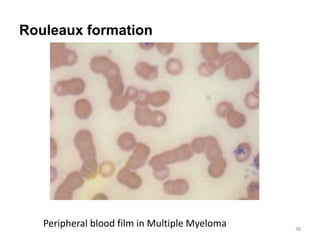
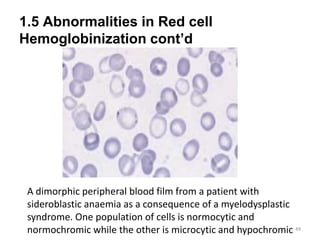
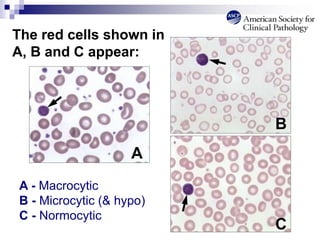
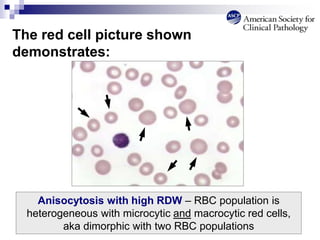
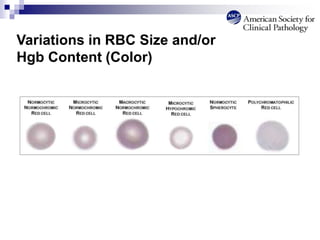
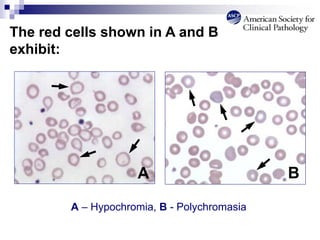
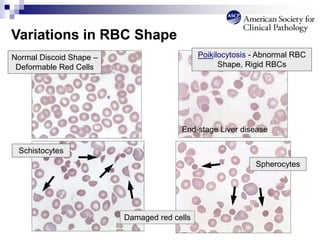
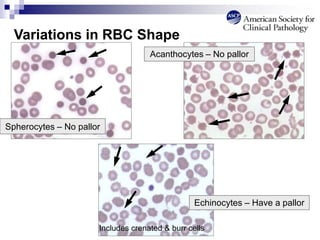
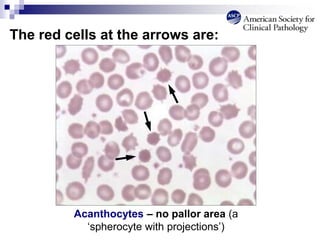
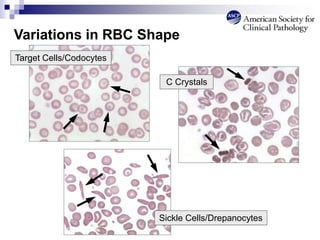
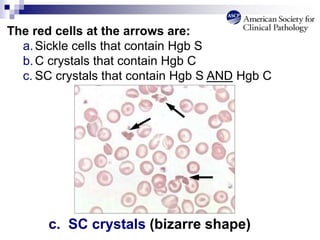
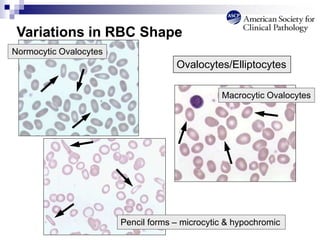
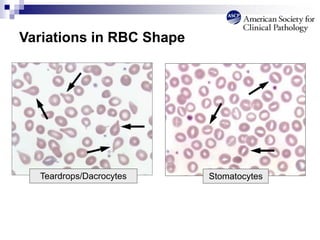
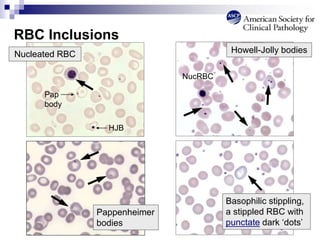
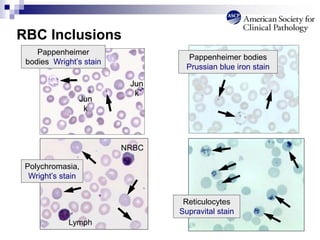
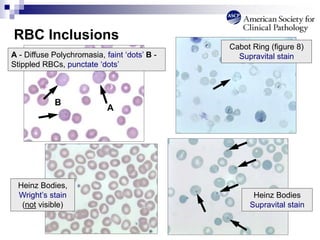
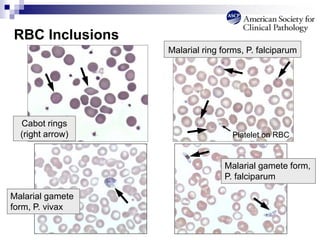
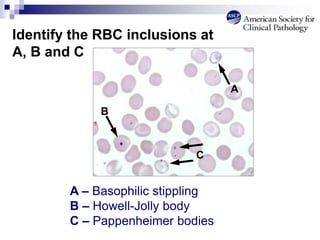
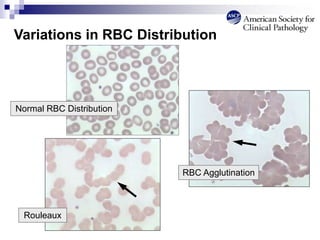
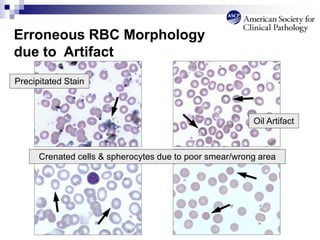
This document provides an overview of red blood cell morphology assessment. It discusses the morphology of normal red blood cells and various abnormal red blood cell forms including variations in size, shape, hemoglobinization, and distribution. Examples of different abnormalities such as macrocytosis, microcytosis, elliptocytes, schistocytes, and rouleaux formation are described. The purpose is to enable students to identify red blood cell abnormalities and correlate them with underlying clinical conditions.





































![Cells and Organs of immune system [Autosaved].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/cellsandorgansofimmunesystemautosaved-260123152717-ea0cb261-thumbnail.jpg?width=640&height=640&fit=bounds)










