PERIPHERAL BLOOD SMEAR (STAINING, CELLS AND CONDITIONS)
This document provides information about drawing and analyzing a peripheral blood smear. It describes the proper technique for making a blood smear, including using a spreader slide to distribute blood in a single layer along the patient slide. An ideal blood smear is described as being uniformly distributed without holes, streaks or waves. The document also outlines the steps for staining a blood smear using Leishman stain, and describes what to look for in the stained smear, such as variations in red blood cell size, shape, and color. Common causes of abnormalities are listed for increased, decreased, or abnormal red blood cells.
PERIPHERAL BLOOD SMEAR (STAINING, CELLS AND CONDITIONS)
1.
PERIPHERAL BLOOD SMEAR
Dr.Roshan Banerjee
1st Year Junior Resident
College Of Medicine and Sagore Dutta Hospital
2.
Drawing a PeripheralBlood Smear
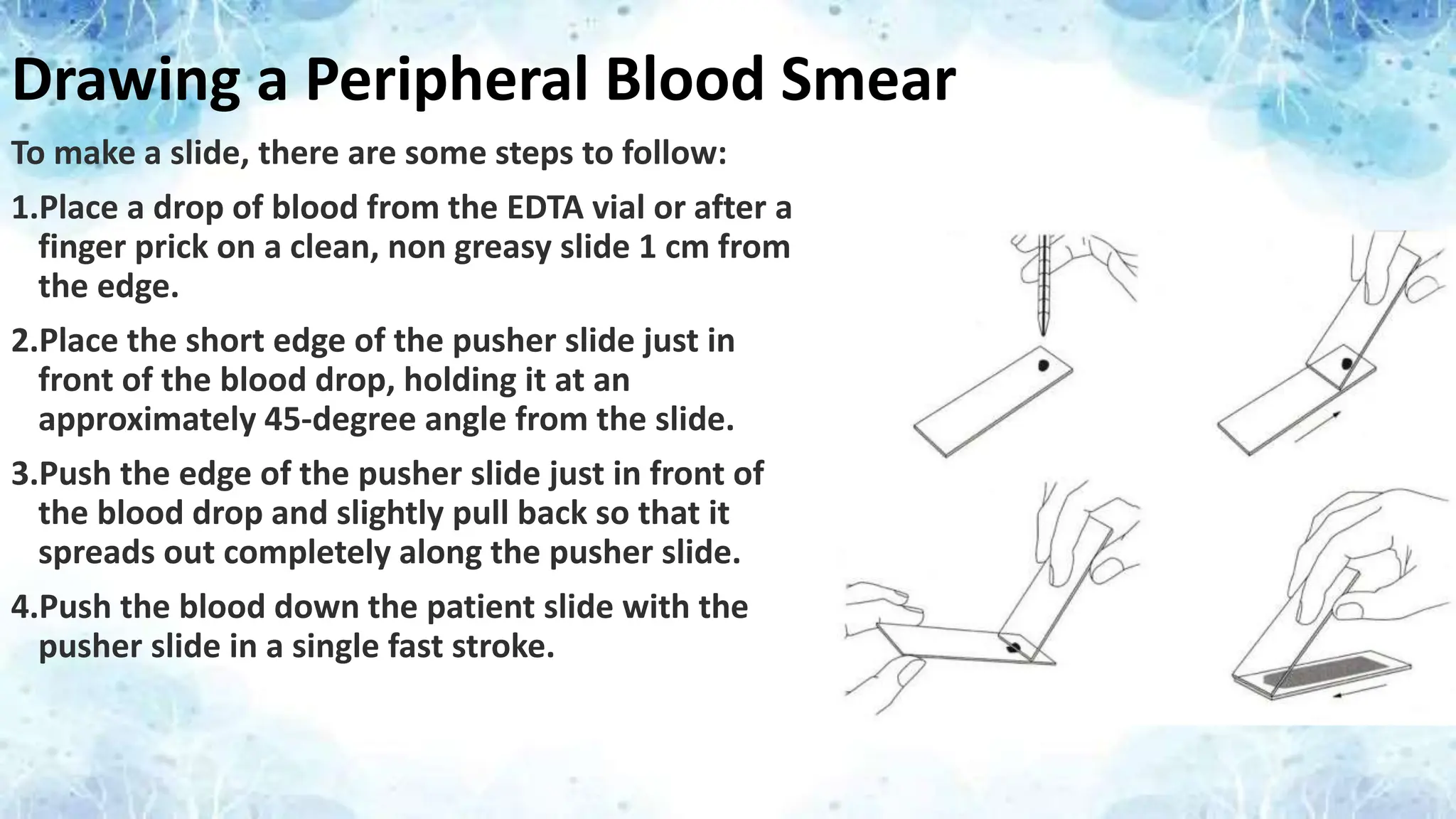
To make a slide, there are some steps to follow:
1.Place a drop of blood from the EDTA vial or after a
finger prick on a clean, non greasy slide 1 cm from
the edge.
2.Place the short edge of the pusher slide just in
front of the blood drop, holding it at an
approximately 45-degree angle from the slide.
3.Push the edge of the pusher slide just in front of
the blood drop and slightly pull back so that it
spreads out completely along the pusher slide.
4.Push the blood down the patient slide with the
pusher slide in a single fast stroke.
3.
Criteria of anIdeal Blood Smear
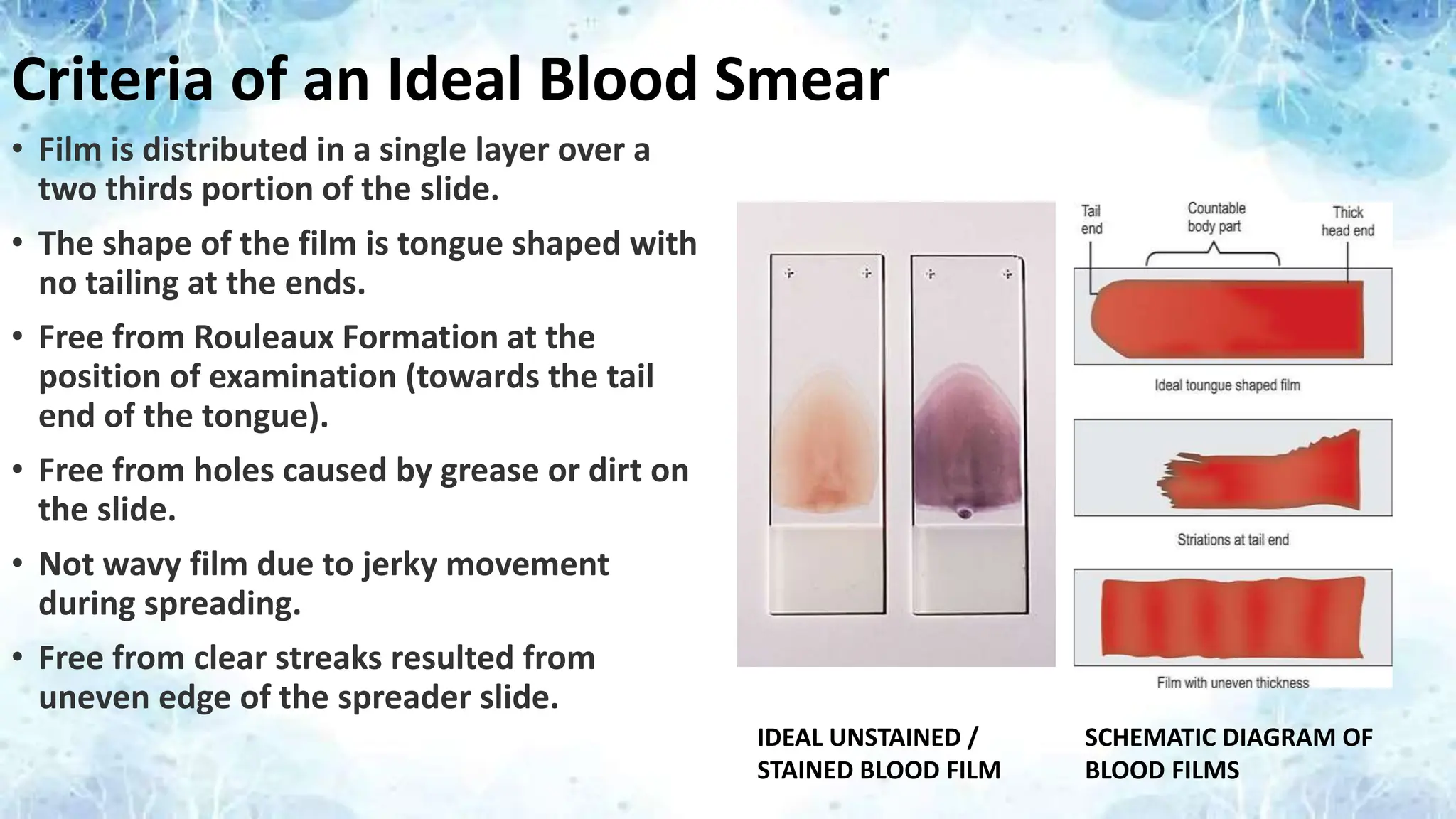
• Film is distributed in a single layer over a
two thirds portion of the slide.
• The shape of the film is tongue shaped with
no tailing at the ends.
• Free from Rouleaux Formation at the
position of examination (towards the tail
end of the tongue).
• Free from holes caused by grease or dirt on
the slide.
• Not wavy film due to jerky movement
during spreading.
• Free from clear streaks resulted from
uneven edge of the spreader slide.
IDEAL UNSTAINED /
STAINED BLOOD FILM
SCHEMATIC DIAGRAM OF
BLOOD FILMS
4.
Staining a PeripheralBlood Smear
• Romanowsky Stains are commonly used for staining Peripheral Blood Films.
• Here we most commonly use Eosinate of Methylene Blue dissolved in Acetone
Free Methyl Alcohol.
• Steps for Staining a Peripheral Blood Smear
• Pour Leishman stain to cover the air dried smear completely and allow to fix
for 2-3 mins.
• Add Buffered Water twice the amount of Leishman stain and allow to stain
for 7-10 mins.
• Appearance of golden scum or sheen on the surface of stain indicates
staining is complete.
• Wash the stain off the slide with running tap water.
• Air dry the slide and view it under a microscope.
5.
Components of LeishmanStain
Eosinate of Methylene Blue : 0.5 gm
Acetone Free Methyl Alcohol : 100 ml
Buffer Water
Solution A
• Potassium Dihydrogen Phosphate : 9.08 g/liter
Solution B
• Dibasic Sodium Phosphate : 9.47 g/liter
Mix Solutions A and B in the following proportion to make 100 ml buffer water for pH 6.8
Solution – 50.8 ml
Solution – 49.2 ml
Red Blood Cells
•Morphology of Normal Red Blood Cells
• Biconcave disc shaped.
• Diameter: 7-8 μm.
• Average volume : 90 fl.
• Central pallor occupy 1/3rd of total size.
• Approx. same as nucleus of mature lymphocyte
• New-born : 4.1–6.1 million/mm3
• Children : 3.6–5.5 million/mm3
• Adult : (Males): 4.6–6.0 million/mm3
• Adult : (Females): 4.2–5.0 million/mm3
• Pregnancy : Slightly lower than normal adult values
8.
Causes of IncreasedRBC Count
• Polycythemia vera (often a hereditary problem)
• Excessive smoking
• High altitudes
• Renal neoplasia (the kidneys are producing too much erythropoietin)
• Heart failure or some heart diseases
• Lung diseases like emphysema, pulmonary fibrosis, etc.
• Dehydration
• Erythropoietin doping by athletes to boost their performance
• Hemoglobinopathies
• Adrenal cortical hyperfunction
• Anabolic metabolism
9.
Causes of DecreasedRBC Count
Broadly, the causes of decreased RBC count may be classified as:
• 1. Impaired red blood cell (RBC) production
• 2. Increased RBC destruction (hemolytic anemias)
• 3. Blood loss
• 4. Fluid overload (Hemodilution)
10.
Decreased RBC countdue to impaired production
• Disturbance of proliferation and differentiation of stem cells:
– Pure red cell aplasia
– Aplastic anemia (affecting all kinds of blood cells)
– Fanconi anemia (a hereditary disorder featuring aplastic anemia and other abnormalities)
– Anemia of renal failure (insufficient erythropoietin production)
– Anemia of endocrine disorders
• Disturbance of proliferation and maturation of erythroblasts:
– Pernicious anemia (macrocytic anemia due to impaired absorption of vitamin B12)
– Anemia of folic acid and vitamin B12 deficiency (megaloblastic anemia)
– Anemia of prematurity (diminished erythropoietin response in premature infants)
– Iron deficiency anemia (resulting in deficient heme synthesis)
– Thalassemias (causing deficient globin synthesis)
– Anemia of renal failure (erythropoietin deficiency)
• Other mechanisms of impaired RBC production:
– Myelodysplastic syndrome
– Anemia of chronic inflammation
– Myelophthisic anemia or Myelophthisis (a severe type of anemia resulting from the replacement of bone marrow
by malignant tumors or granulomas)
11.
Decreased RBC countdue to increased destruction :
(Hemolytic Disorders)
(A) Intrinsic (intracorpuscular) abnormalities
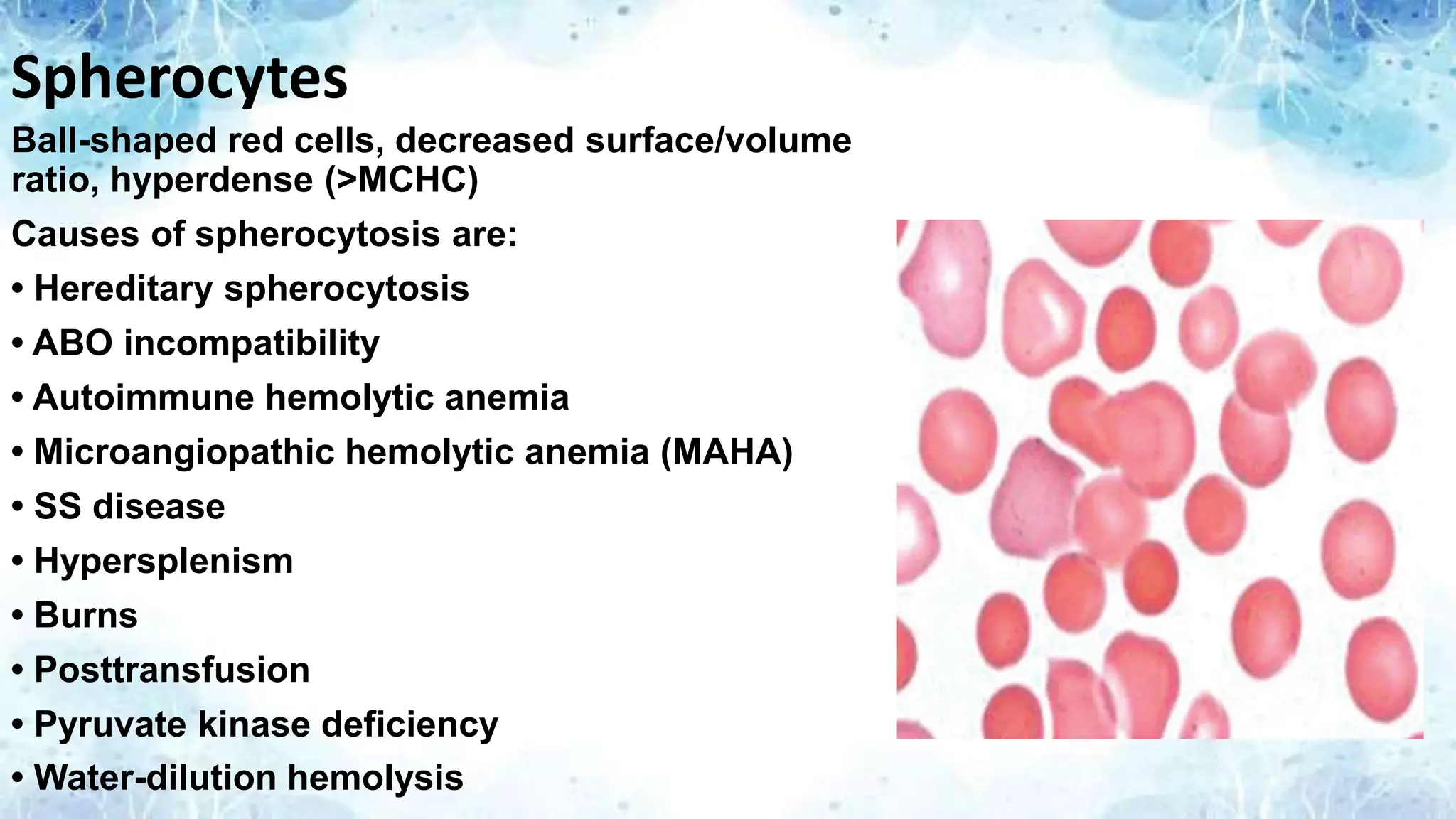
• Membrane Disruption - Hereditary spherocytosis (a hereditary membrane defect, causing RBC to be sequestered by the spleen),
Hereditary elliptocytosis(defect in membrane skeleton proteins), Abetalipoproteinemia (causing defects in membrane lipids)
• Enzyme deficiencies – Pyruvate kinase and hexokinase deficiencies (causing defective glycolysis) and Glucose-6-phosphate
dehydrogenase deficiency (causing increased oxidative stress)
• Hemoglobinopathies – Sickle cell anemia, Hemoglobinopathies causing unstable hemoglobins and Paroxysmal nocturnal
hemoglobinuria
(B) Extrinsic (extracorpuscular) abnormalities
• Antibody-mediated
– Warm autoimmune hemolytic anemia is an anemia caused by autoimmune attack against red blood cells, primarily by IgG. It is the
most common of the autoimmune hemolytic diseases. It can be idiopathic, drug-associated or secondary to systemic lupus
erythematosus, or a malignancy, such as chronic lymphocytic leukemia (CLL)
– Cold agglutinin hemolytic anemia (IgM mediated,can be idiopathic or secondary)
– Hemolytic disease of the newborn
– Mismatch transfusion reactions
• Mechanical trauma to red cells
– Microangiopathic hemolytic anemias including TTP, HUS
– Disseminated intravascular coagulation (DIC)
– Infections, including malaria
– Prosthetic valve/heart surgery
12.
Decreased RBC countdue to blood loss
• Trauma or surgery, causing acute blood loss
• Gastrointestinal tract lesions (causing chronic blood loss)
• Gynecologic disturbances (also generally causing chronic blood loss)
• Hypervolemia causes spurious low RBC count (due to hemodilution)
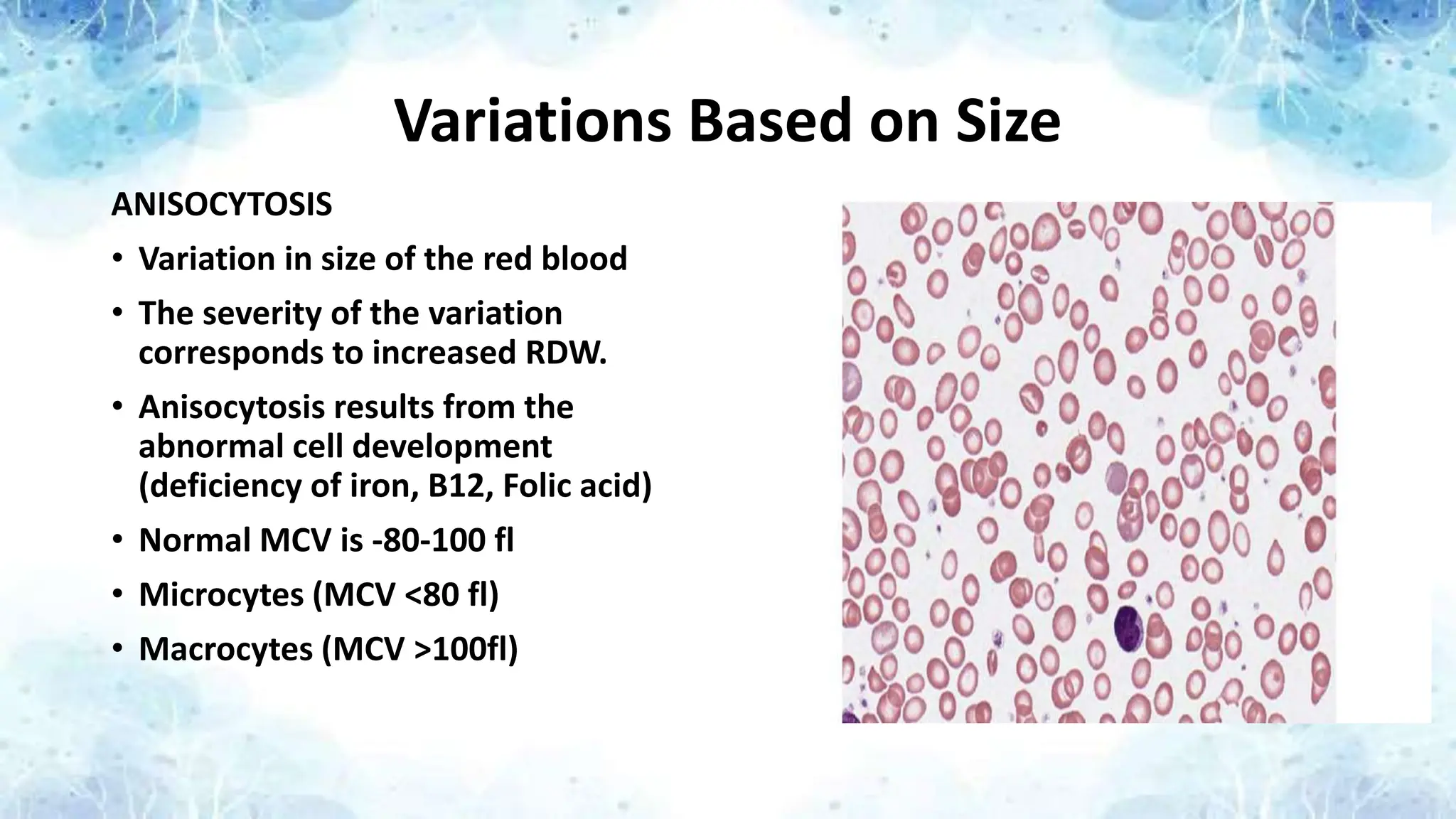
Variations Based onSize
ANISOCYTOSIS
• Variation in size of the red blood
• The severity of the variation
corresponds to increased RDW.
• Anisocytosis results from the
abnormal cell development
(deficiency of iron, B12, Folic acid)
• Normal MCV is -80-100 fl
• Microcytes (MCV <80 fl)
• Macrocytes (MCV >100fl)
15.
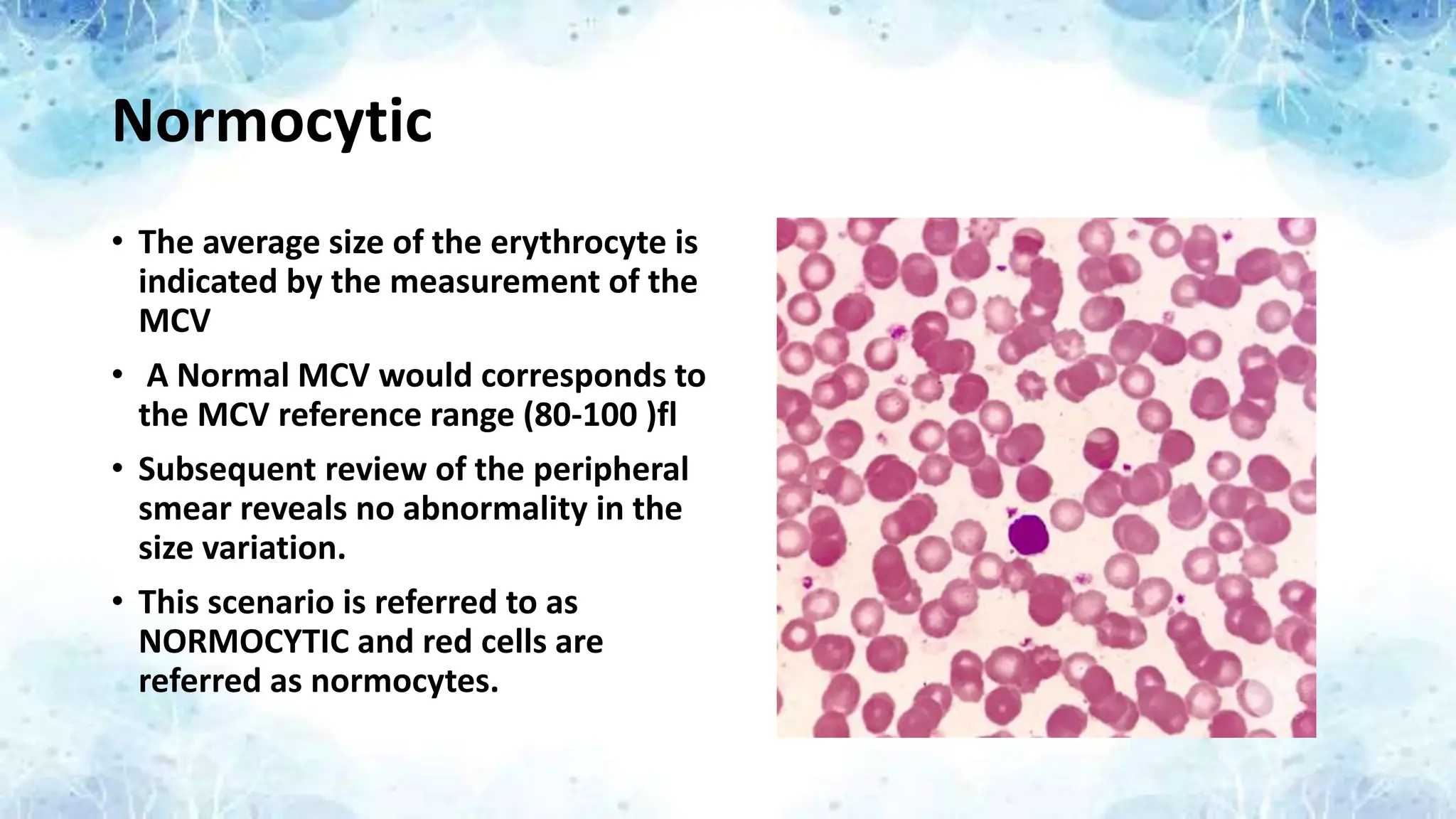
Normocytic
• The averagesize of the erythrocyte is
indicated by the measurement of the
MCV
• A Normal MCV would corresponds to
the MCV reference range (80-100 )fl
• Subsequent review of the peripheral
smear reveals no abnormality in the
size variation.
• This scenario is referred to as
NORMOCYTIC and red cells are
referred as normocytes.
16.
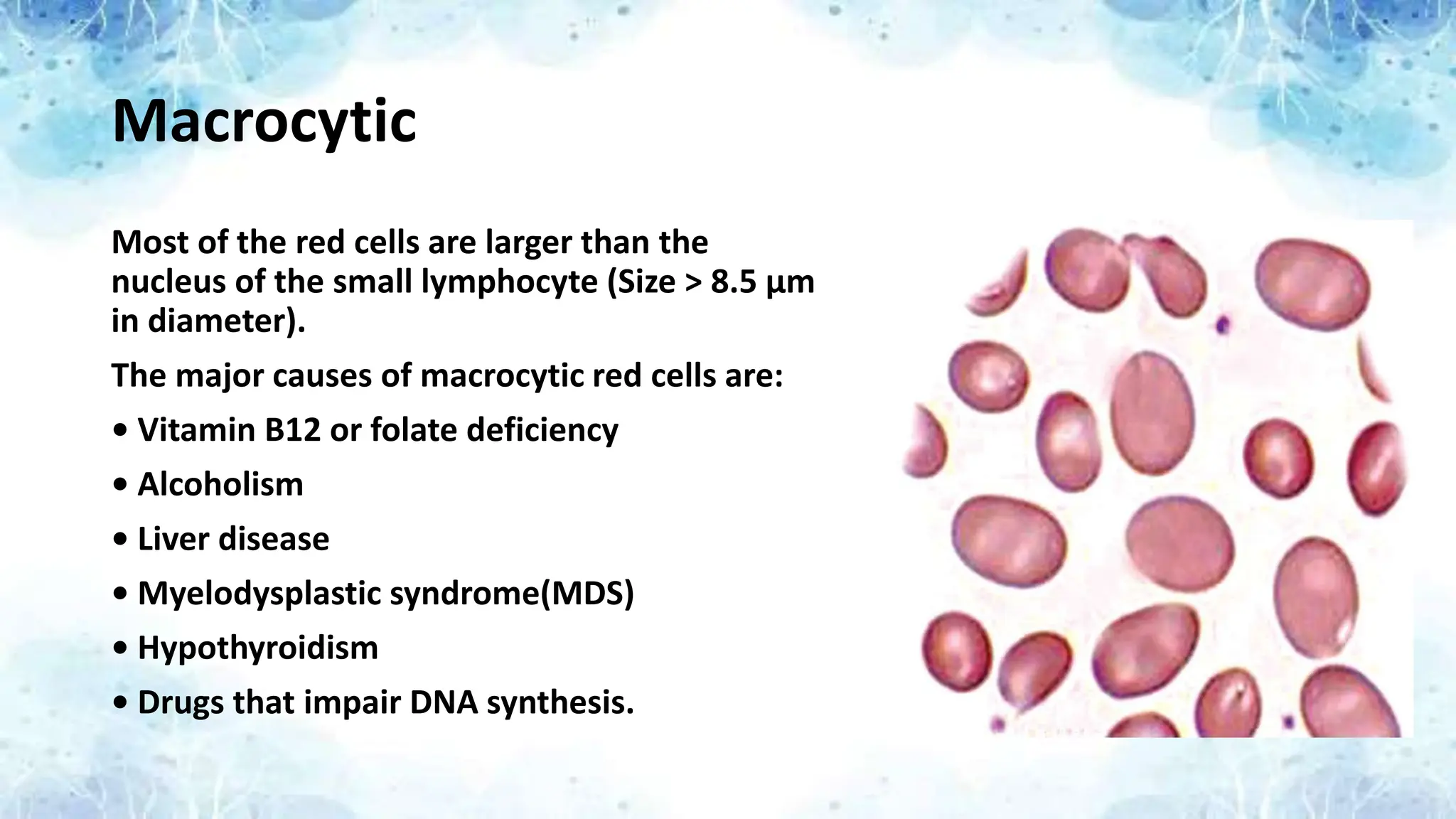
Macrocytic
Most of thered cells are larger than the
nucleus of the small lymphocyte (Size > 8.5 μm
in diameter).
The major causes of macrocytic red cells are:
• Vitamin B12 or folate deficiency
• Alcoholism
• Liver disease
• Myelodysplastic syndrome(MDS)
• Hypothyroidism
• Drugs that impair DNA synthesis.
17.
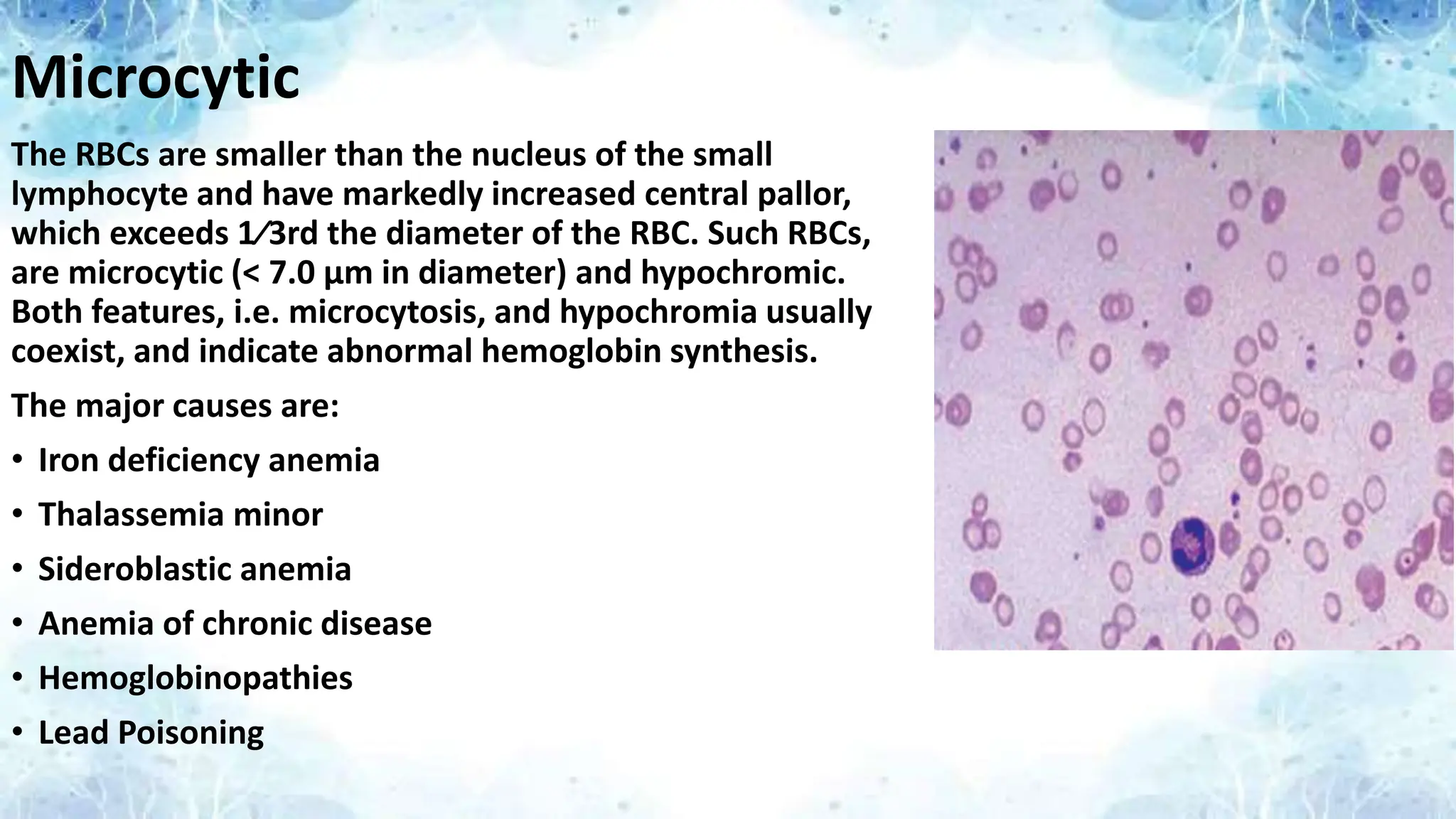
Microcytic
The RBCs aresmaller than the nucleus of the small
lymphocyte and have markedly increased central pallor,
which exceeds 1⁄3rd the diameter of the RBC. Such RBCs,
are microcytic (< 7.0 μm in diameter) and hypochromic.
Both features, i.e. microcytosis, and hypochromia usually
coexist, and indicate abnormal hemoglobin synthesis.
The major causes are:
• Iron deficiency anemia
• Thalassemia minor
• Sideroblastic anemia
• Anemia of chronic disease
• Hemoglobinopathies
• Lead Poisoning
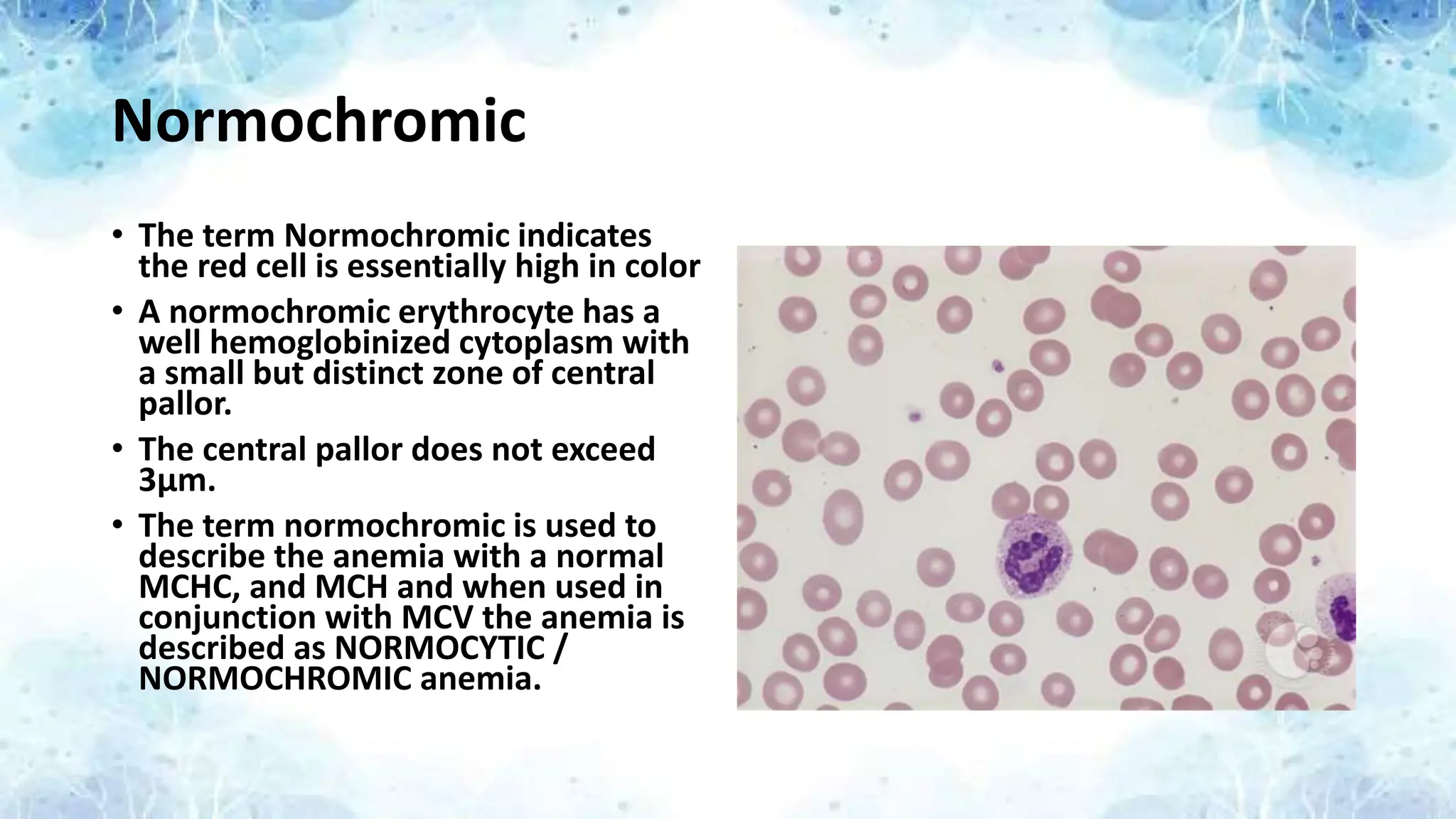
Normochromic
• The termNormochromic indicates
the red cell is essentially high in color
• A normochromic erythrocyte has a
well hemoglobinized cytoplasm with
a small but distinct zone of central
pallor.
• The central pallor does not exceed
3μm.
• The term normochromic is used to
describe the anemia with a normal
MCHC, and MCH and when used in
conjunction with MCV the anemia is
described as NORMOCYTIC /
NORMOCHROMIC anemia.
20.
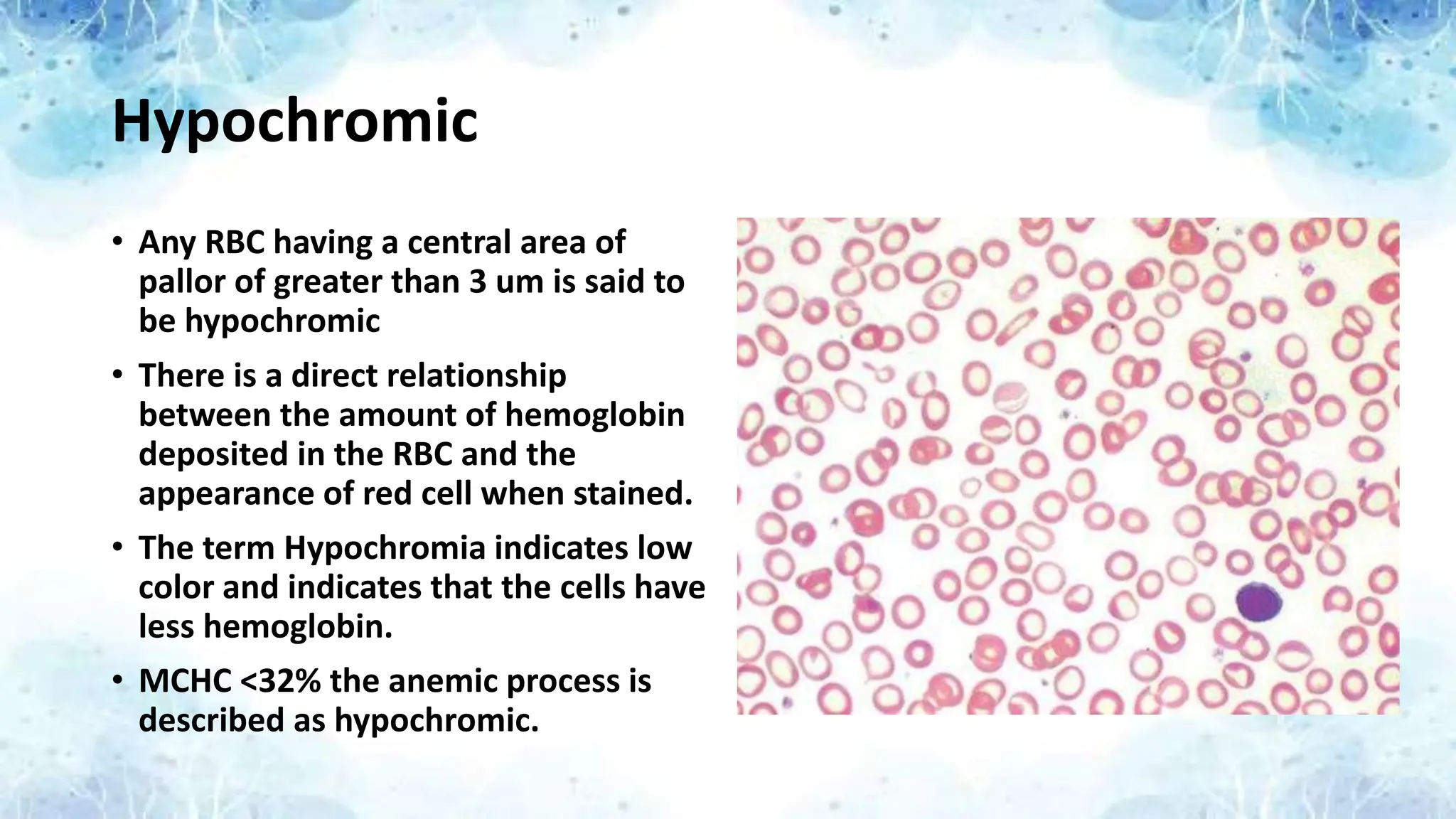
Hypochromic
• Any RBChaving a central area of
pallor of greater than 3 um is said to
be hypochromic
• There is a direct relationship
between the amount of hemoglobin
deposited in the RBC and the
appearance of red cell when stained.
• The term Hypochromia indicates low
color and indicates that the cells have
less hemoglobin.
• MCHC <32% the anemic process is
described as hypochromic.
21.
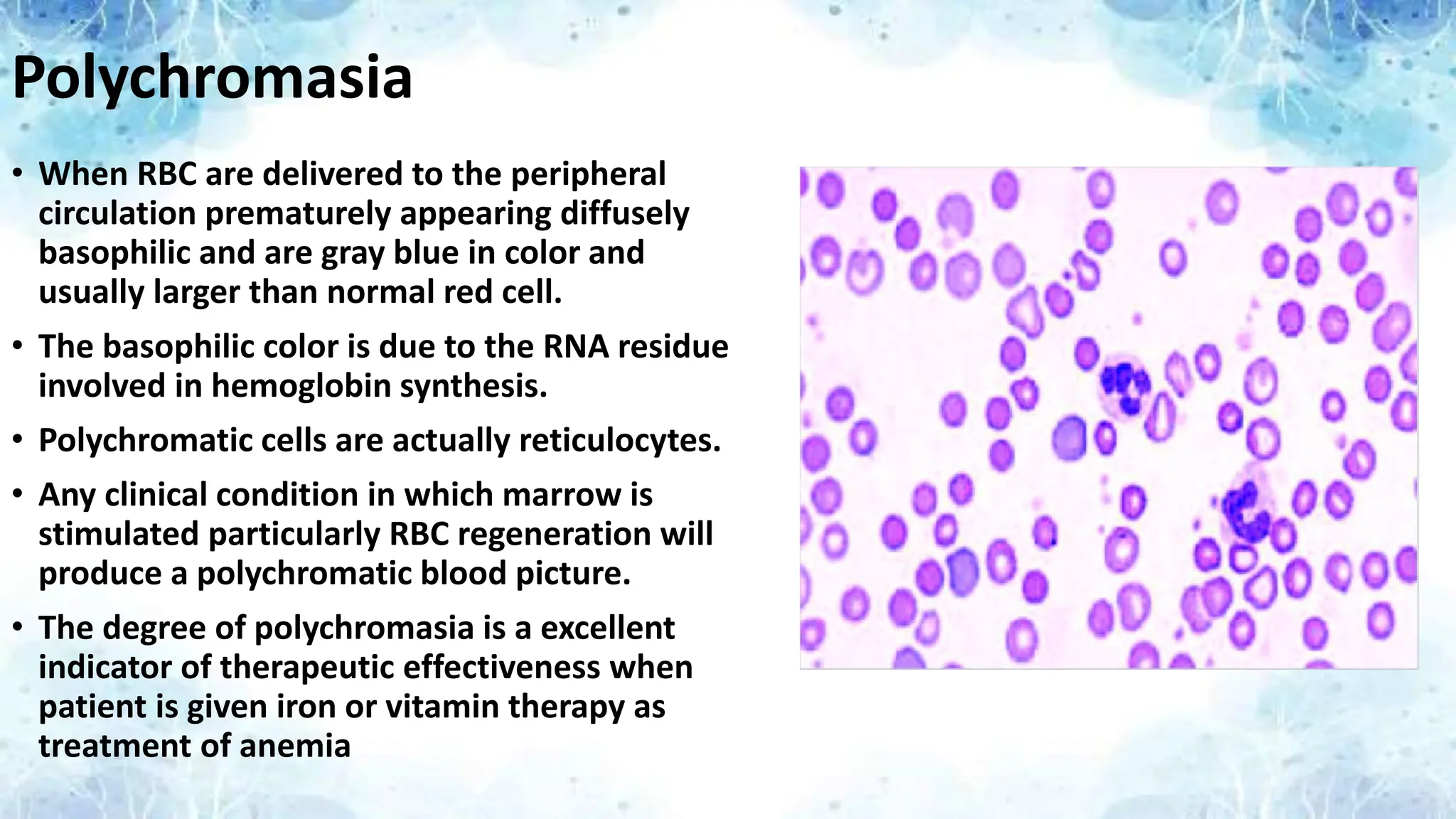
Polychromasia
• When RBCare delivered to the peripheral
circulation prematurely appearing diffusely
basophilic and are gray blue in color and
usually larger than normal red cell.
• The basophilic color is due to the RNA residue
involved in hemoglobin synthesis.
• Polychromatic cells are actually reticulocytes.
• Any clinical condition in which marrow is
stimulated particularly RBC regeneration will
produce a polychromatic blood picture.
• The degree of polychromasia is a excellent
indicator of therapeutic effectiveness when
patient is given iron or vitamin therapy as
treatment of anemia
22.
Variations Based onShape
POIKILOCYTOSIS
Variation In shape is called Poikilocytosis.
It is of following types
• Target cells
• Tear Drop Cells
• Spherocytes
• Echinocytes (Burr Cells)
• Bite cells
23.
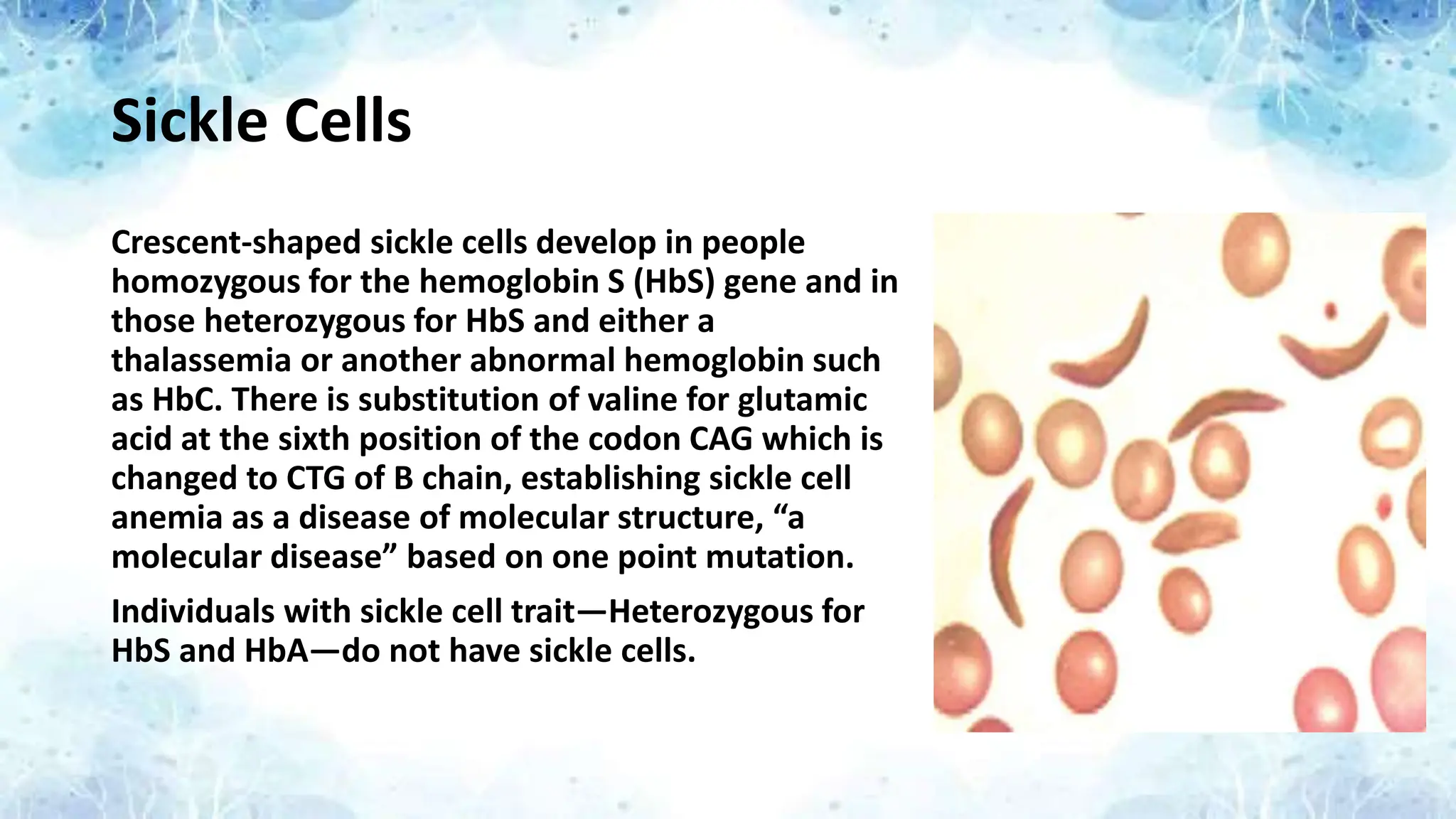
Sickle Cells
Crescent-shaped sicklecells develop in people
homozygous for the hemoglobin S (HbS) gene and in
those heterozygous for HbS and either a
thalassemia or another abnormal hemoglobin such
as HbC. There is substitution of valine for glutamic
acid at the sixth position of the codon CAG which is
changed to CTG of B chain, establishing sickle cell
anemia as a disease of molecular structure, “a
molecular disease” based on one point mutation.
Individuals with sickle cell trait—Heterozygous for
HbS and HbA—do not have sickle cells.
24.
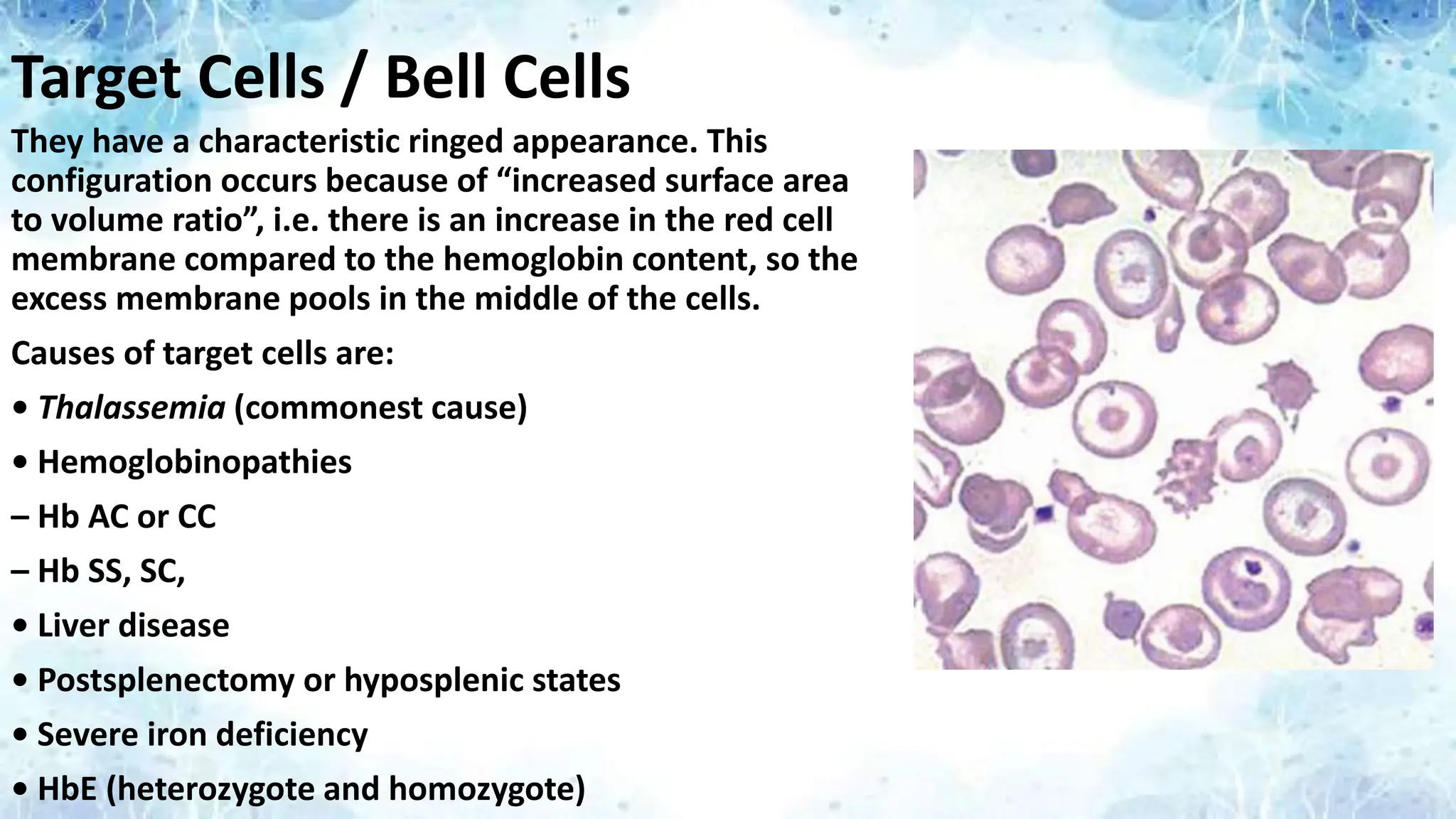
Target Cells /Bell Cells
They have a characteristic ringed appearance. This
configuration occurs because of “increased surface area
to volume ratio”, i.e. there is an increase in the red cell
membrane compared to the hemoglobin content, so the
excess membrane pools in the middle of the cells.
Causes of target cells are:
• Thalassemia (commonest cause)
• Hemoglobinopathies
– Hb AC or CC
– Hb SS, SC,
• Liver disease
• Postsplenectomy or hyposplenic states
• Severe iron deficiency
• HbE (heterozygote and homozygote)
25.
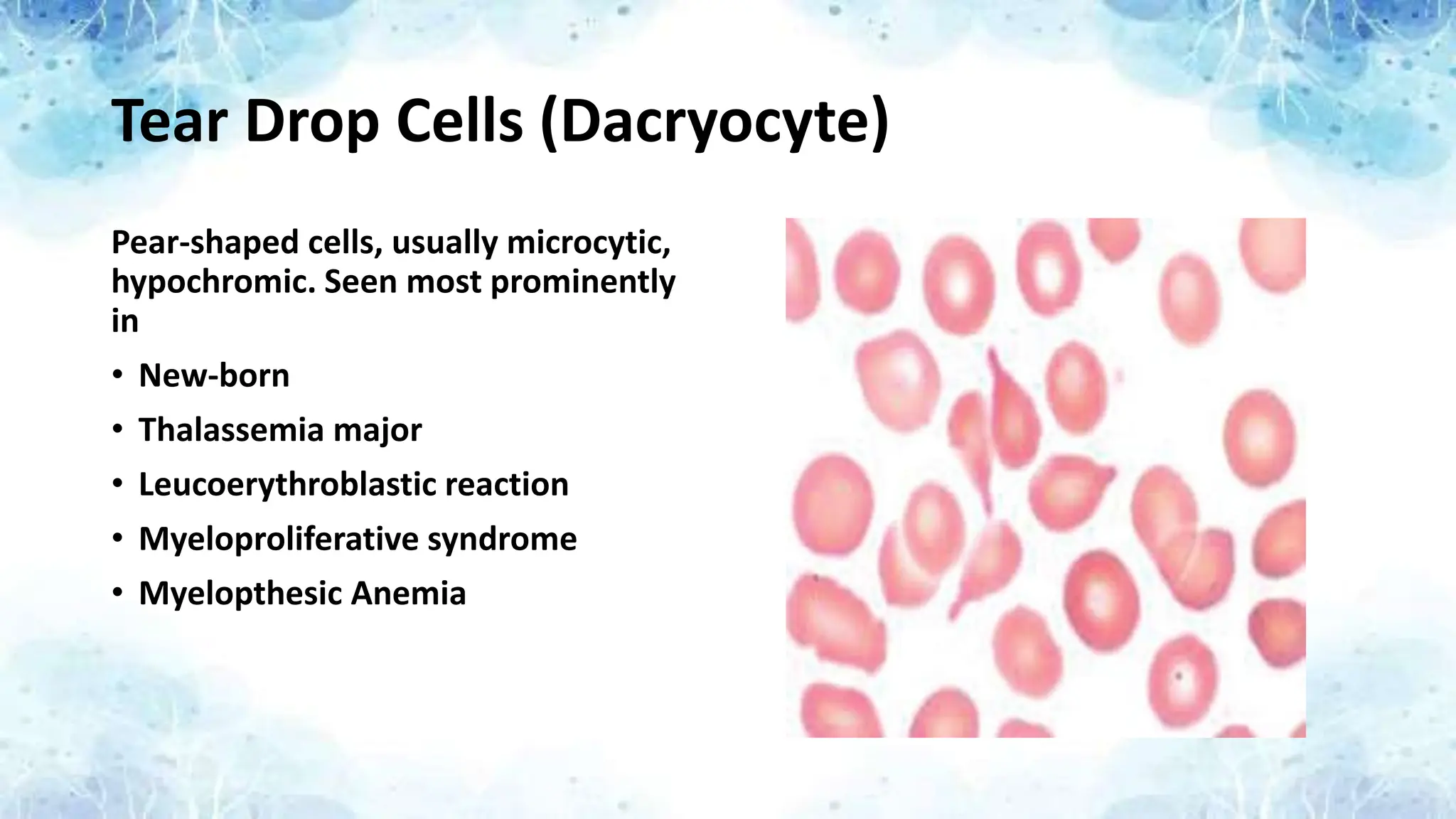
Tear Drop Cells(Dacryocyte)
Pear-shaped cells, usually microcytic,
hypochromic. Seen most prominently
in
• New-born
• Thalassemia major
• Leucoerythroblastic reaction
• Myeloproliferative syndrome
• Myelopthesic Anemia
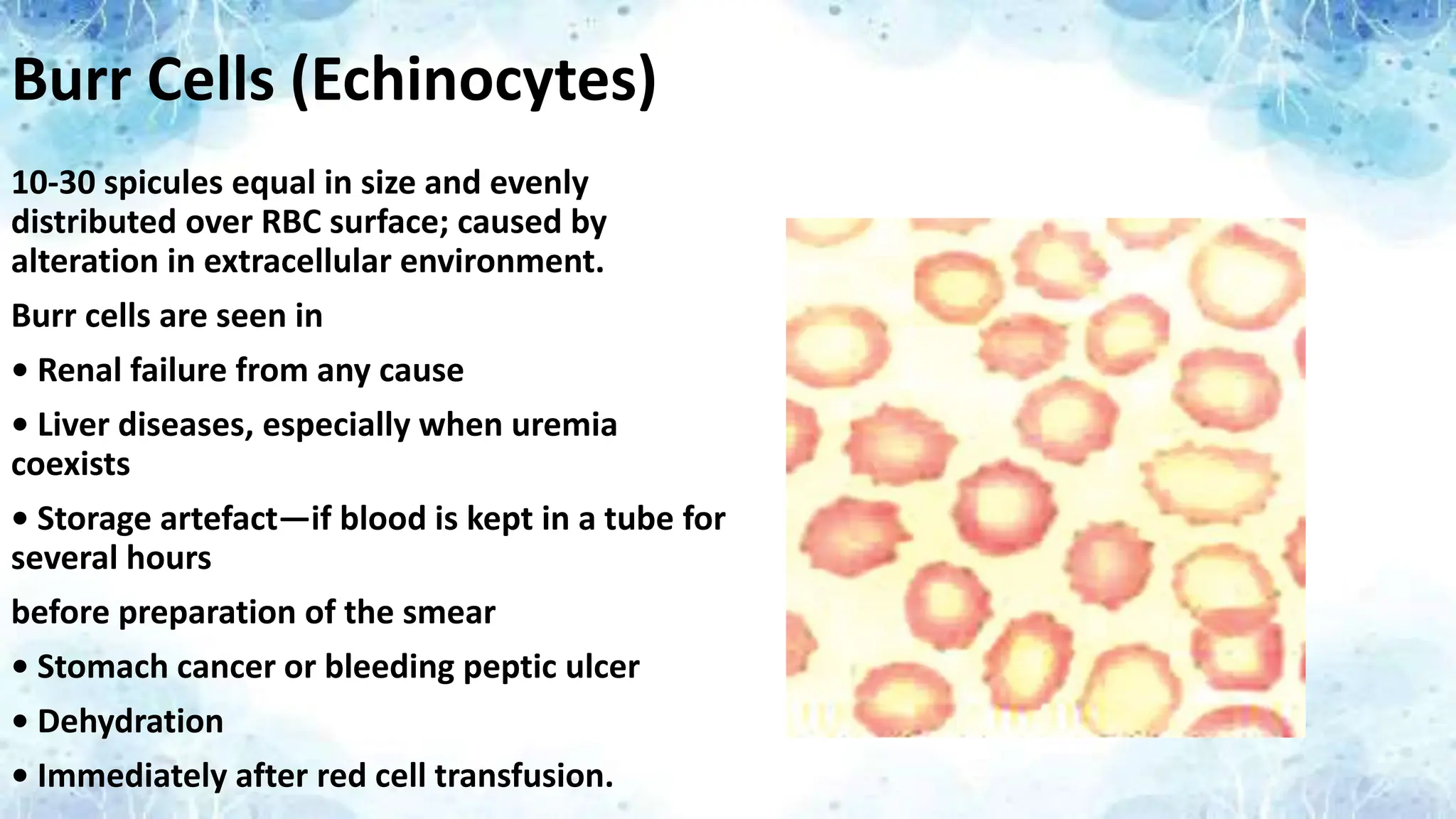
Burr Cells (Echinocytes)
10-30spicules equal in size and evenly
distributed over RBC surface; caused by
alteration in extracellular environment.
Burr cells are seen in
• Renal failure from any cause
• Liver diseases, especially when uremia
coexists
• Storage artefact—if blood is kept in a tube for
several hours
before preparation of the smear
• Stomach cancer or bleeding peptic ulcer
• Dehydration
• Immediately after red cell transfusion.
28.
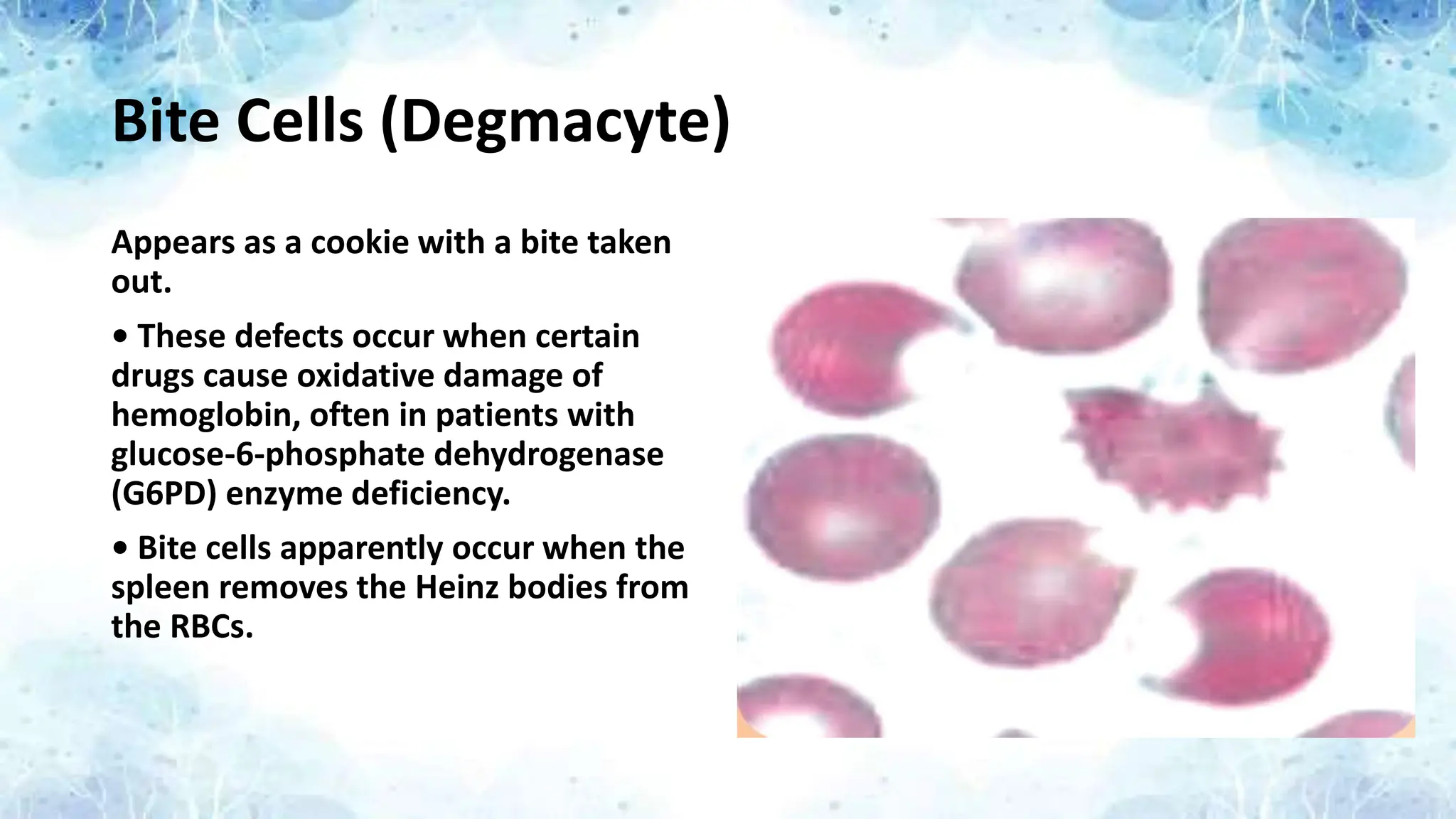
Bite Cells (Degmacyte)
Appearsas a cookie with a bite taken
out.
• These defects occur when certain
drugs cause oxidative damage of
hemoglobin, often in patients with
glucose-6-phosphate dehydrogenase
(G6PD) enzyme deficiency.
• Bite cells apparently occur when the
spleen removes the Heinz bodies from
the RBCs.
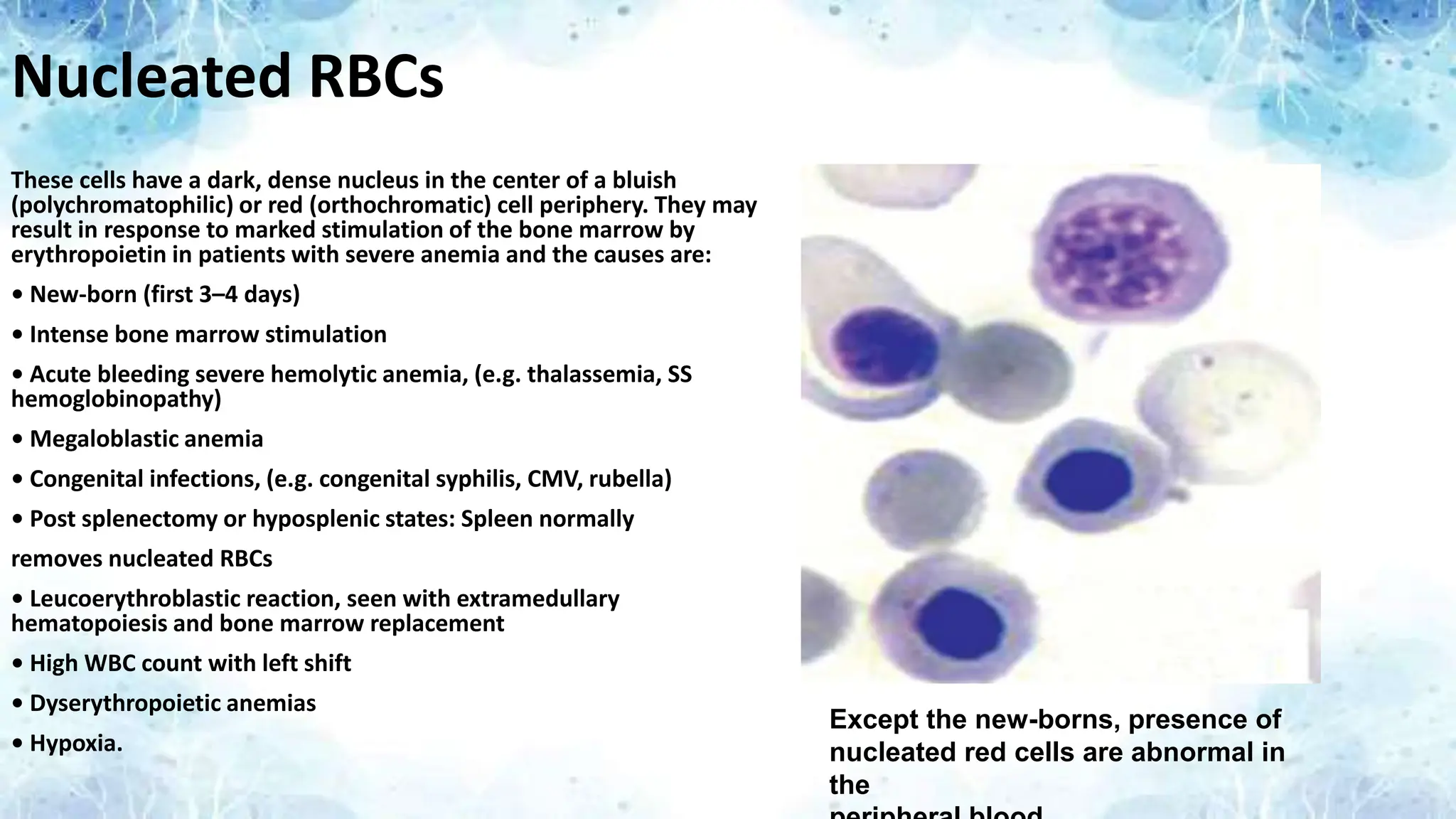
Nucleated RBCs
These cellshave a dark, dense nucleus in the center of a bluish
(polychromatophilic) or red (orthochromatic) cell periphery. They may
result in response to marked stimulation of the bone marrow by
erythropoietin in patients with severe anemia and the causes are:
• New-born (first 3–4 days)
• Intense bone marrow stimulation
• Acute bleeding severe hemolytic anemia, (e.g. thalassemia, SS
hemoglobinopathy)
• Megaloblastic anemia
• Congenital infections, (e.g. congenital syphilis, CMV, rubella)
• Post splenectomy or hyposplenic states: Spleen normally
removes nucleated RBCs
• Leucoerythroblastic reaction, seen with extramedullary
hematopoiesis and bone marrow replacement
• High WBC count with left shift
• Dyserythropoietic anemias
• Hypoxia.
Except the new-borns, presence of
nucleated red cells are abnormal in
the
31.
Howell – JollyBodies
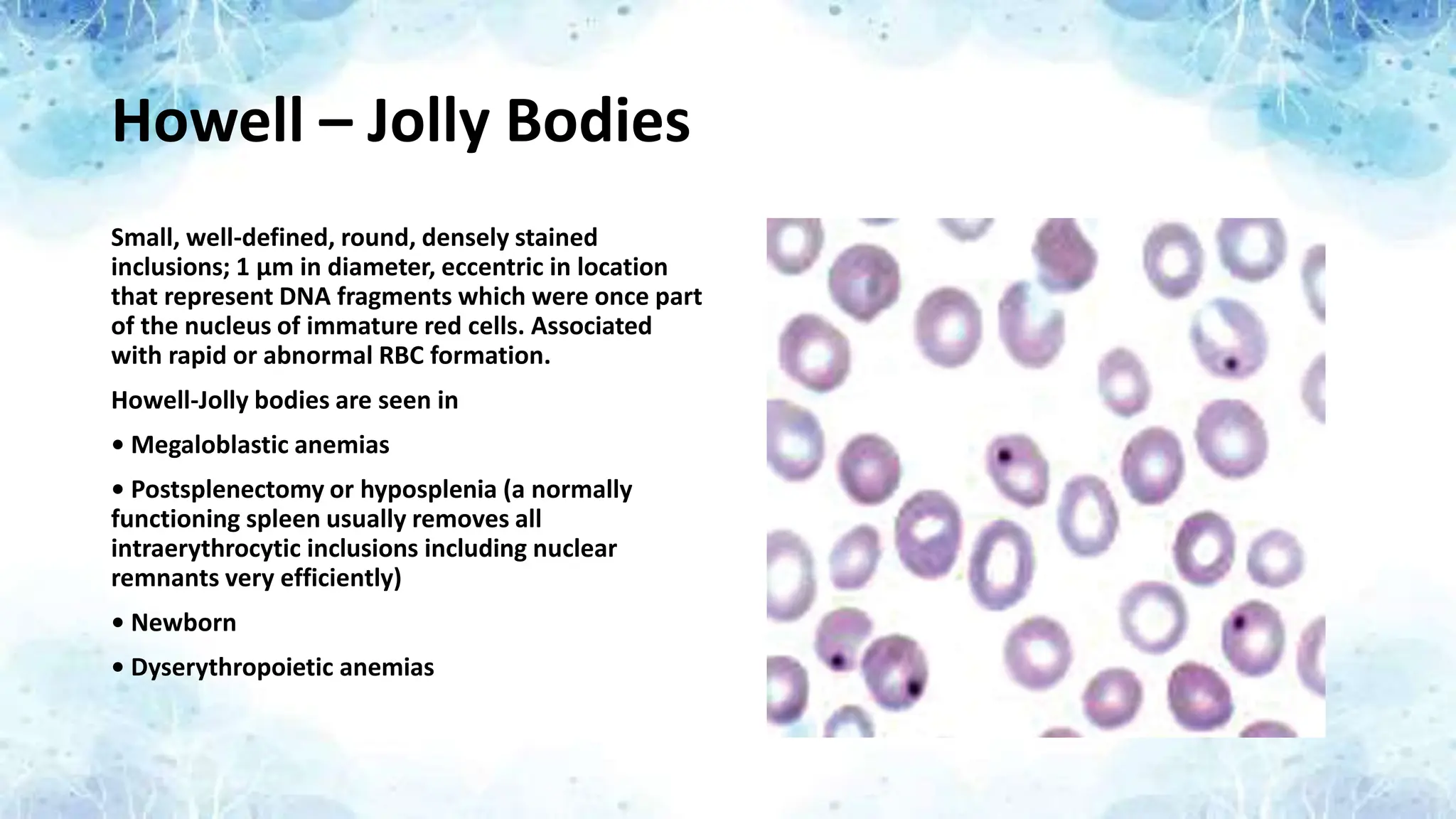
Small, well-defined, round, densely stained
inclusions; 1 μm in diameter, eccentric in location
that represent DNA fragments which were once part
of the nucleus of immature red cells. Associated
with rapid or abnormal RBC formation.
Howell-Jolly bodies are seen in
• Megaloblastic anemias
• Postsplenectomy or hyposplenia (a normally
functioning spleen usually removes all
intraerythrocytic inclusions including nuclear
remnants very efficiently)
• Newborn
• Dyserythropoietic anemias
32.
Heinz Bodies
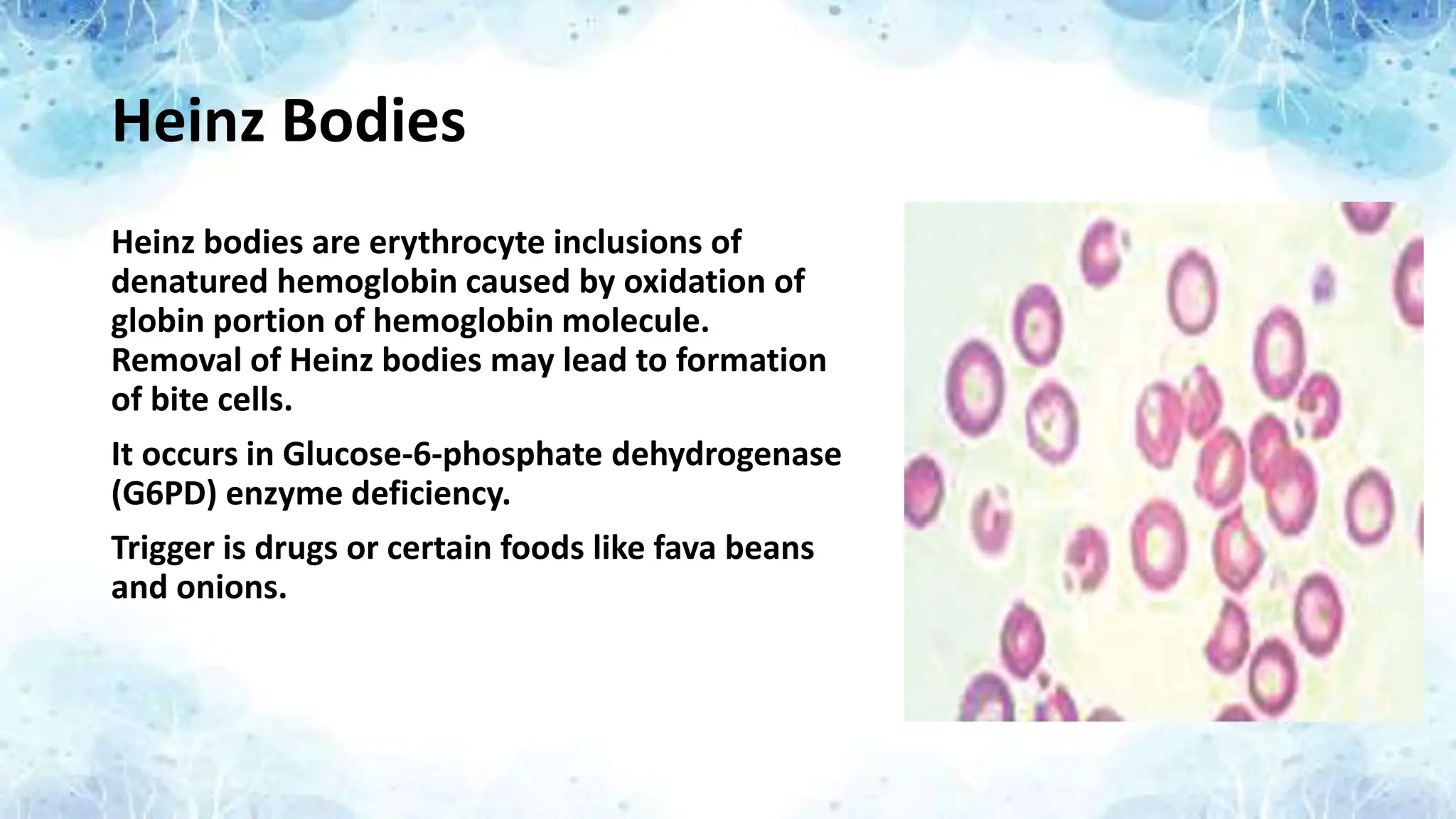
Heinz bodiesare erythrocyte inclusions of
denatured hemoglobin caused by oxidation of
globin portion of hemoglobin molecule.
Removal of Heinz bodies may lead to formation
of bite cells.
It occurs in Glucose-6-phosphate dehydrogenase
(G6PD) enzyme deficiency.
Trigger is drugs or certain foods like fava beans
and onions.
33.
Basophilic Stippling
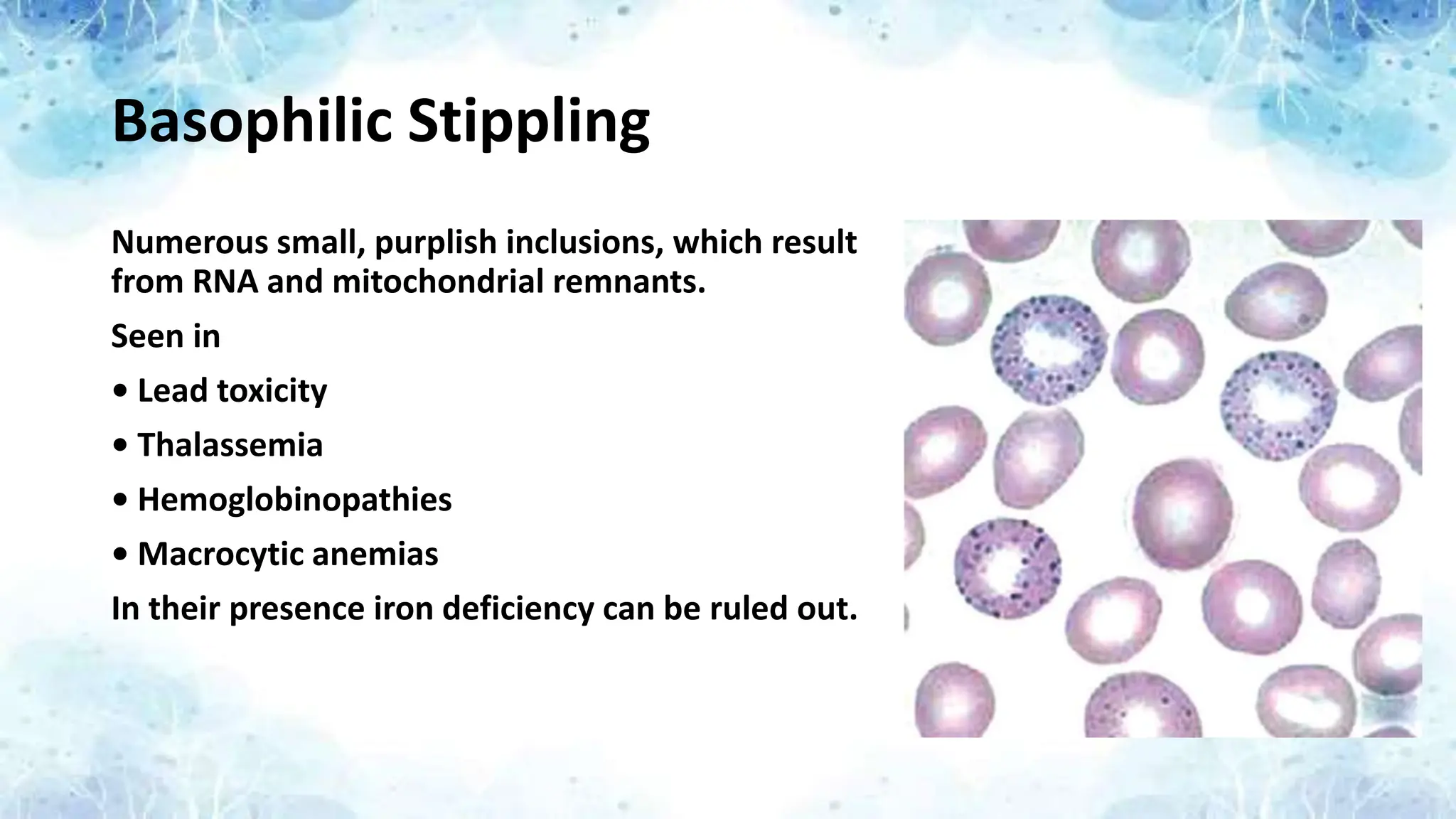
Numerous small,purplish inclusions, which result
from RNA and mitochondrial remnants.
Seen in
• Lead toxicity
• Thalassemia
• Hemoglobinopathies
• Macrocytic anemias
In their presence iron deficiency can be ruled out.
34.
Cabot Rings
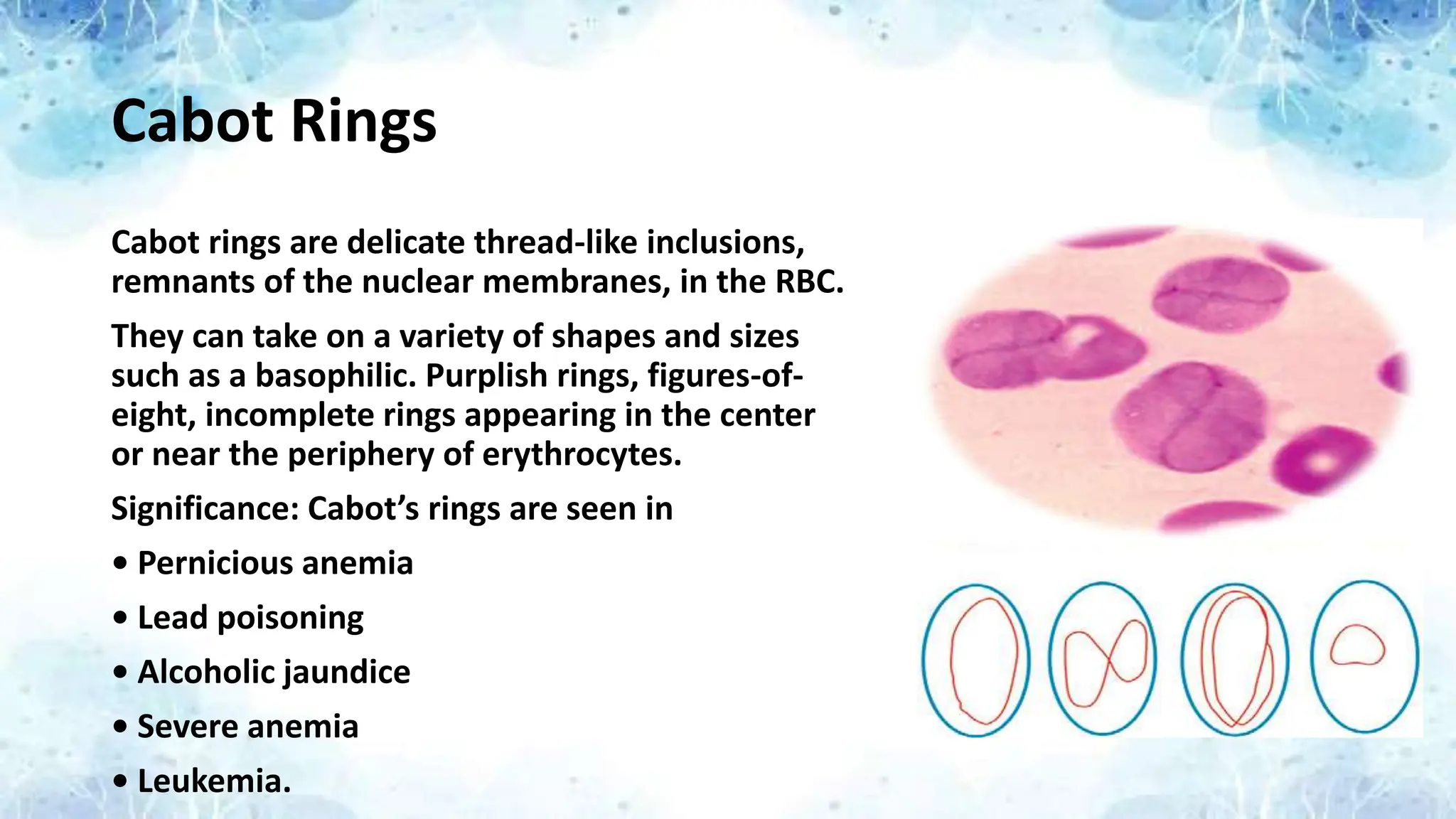
Cabot ringsare delicate thread-like inclusions,
remnants of the nuclear membranes, in the RBC.
They can take on a variety of shapes and sizes
such as a basophilic. Purplish rings, figures-of-
eight, incomplete rings appearing in the center
or near the periphery of erythrocytes.
Significance: Cabot’s rings are seen in
• Pernicious anemia
• Lead poisoning
• Alcoholic jaundice
• Severe anemia
• Leukemia.
35.
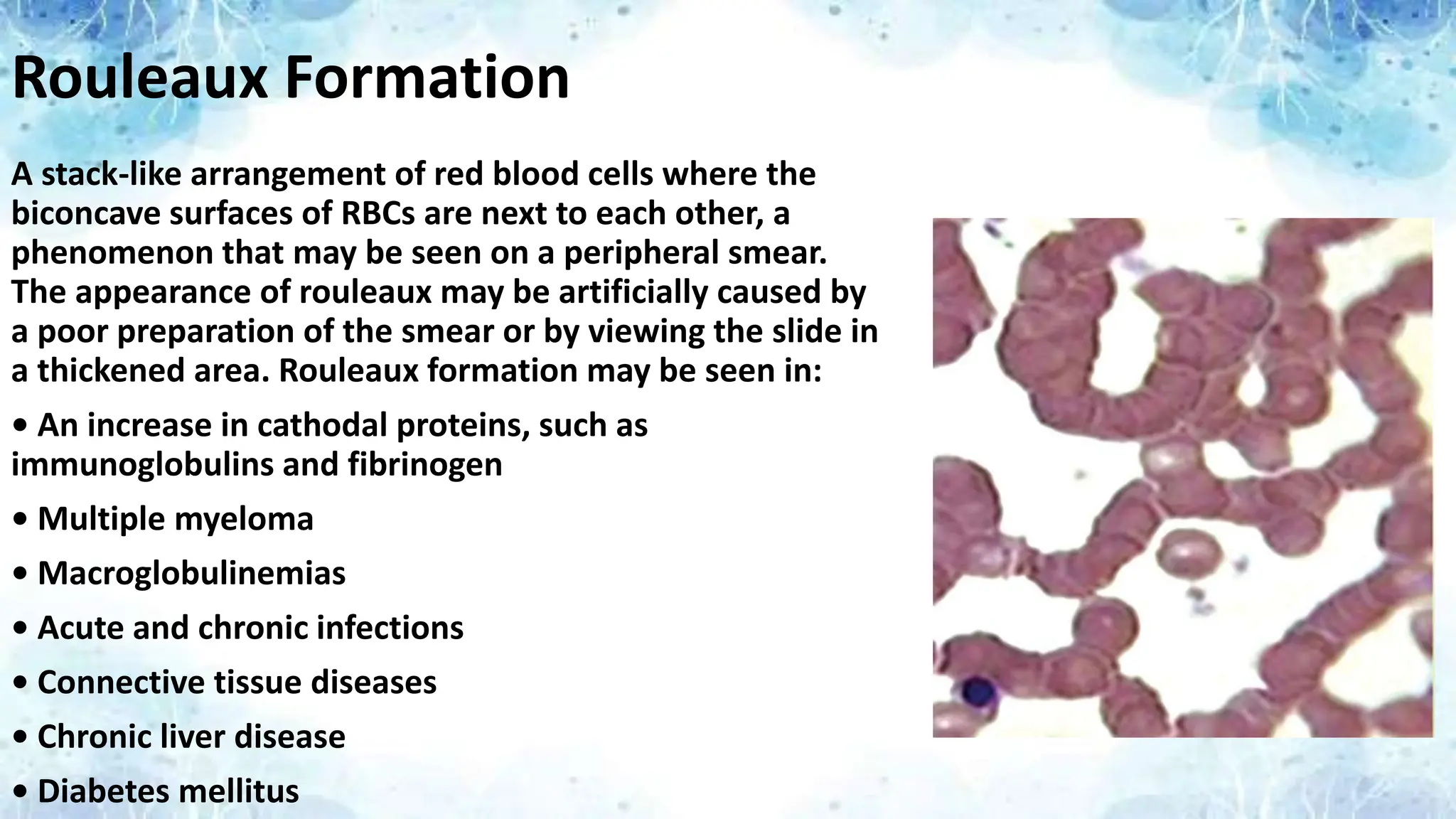
Rouleaux Formation
A stack-likearrangement of red blood cells where the
biconcave surfaces of RBCs are next to each other, a
phenomenon that may be seen on a peripheral smear.
The appearance of rouleaux may be artificially caused by
a poor preparation of the smear or by viewing the slide in
a thickened area. Rouleaux formation may be seen in:
• An increase in cathodal proteins, such as
immunoglobulins and fibrinogen
• Multiple myeloma
• Macroglobulinemias
• Acute and chronic infections
• Connective tissue diseases
• Chronic liver disease
• Diabetes mellitus
Total Count andDifferential Count of White
Blood Cells from a Peripheral Blood Smear
• The Total Count of WBC estimate can be performed using a factor which is
based on the fact that WBC seen in 40x is approx. equivalent to 2000
cells/micro liter.
• Counting of the WBCs is done in a Zig Zag motion from the zone of examination
of the smear.
• For example if the average number of WBC counted per high power field (HPF)
is 5, the estimate Total Count of WBC is 5 x 2000 = 10000. (An average from 10
HPF examinations is usually taken)
• Differential Count can be estimated from the above factor by counting the
different types of WBCs in an high power field and respectively multiplying it
with a factor of 2000. The Respective Percentage of Differential Count can be
calculated mathematically with the data.
38.
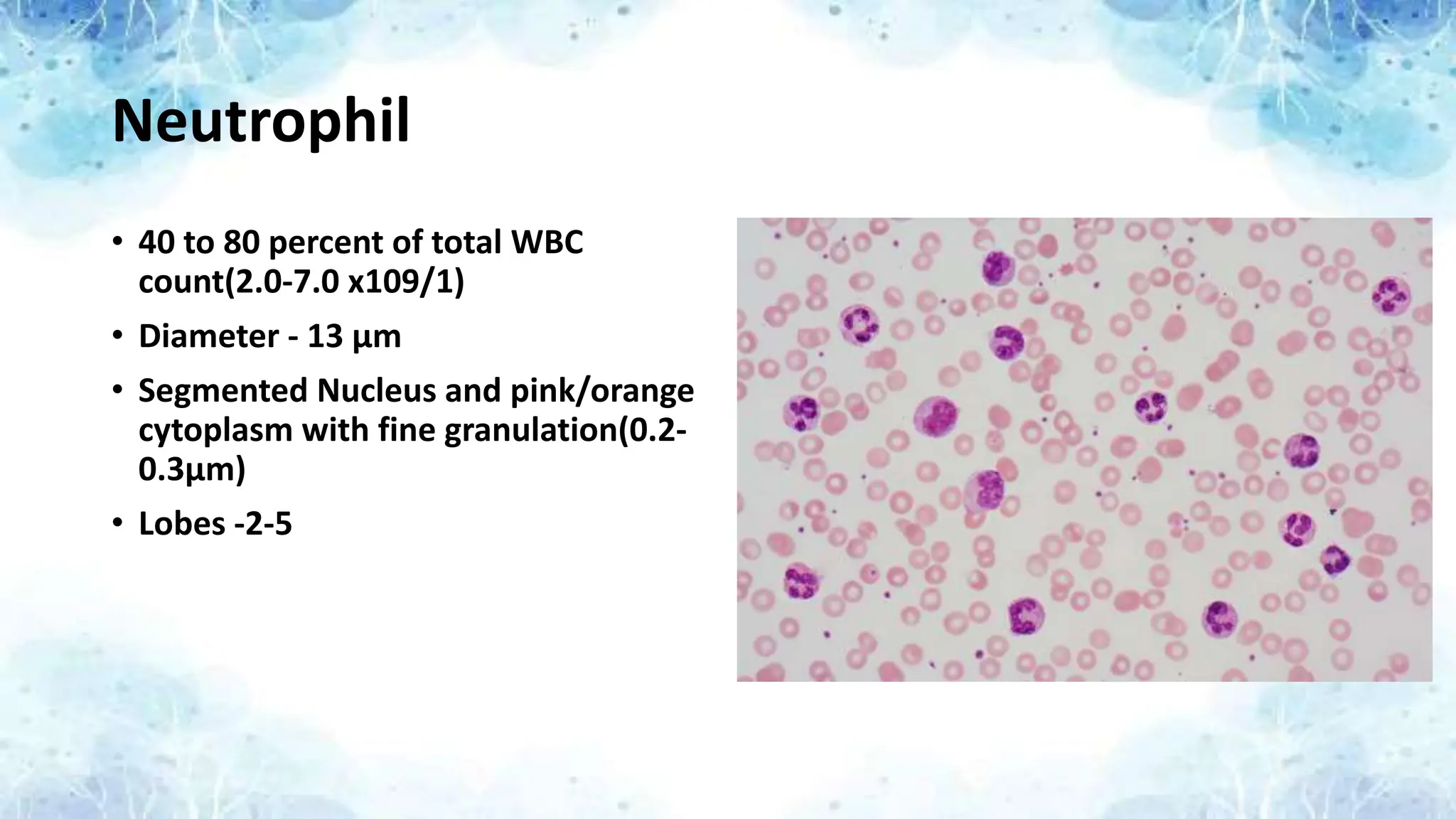
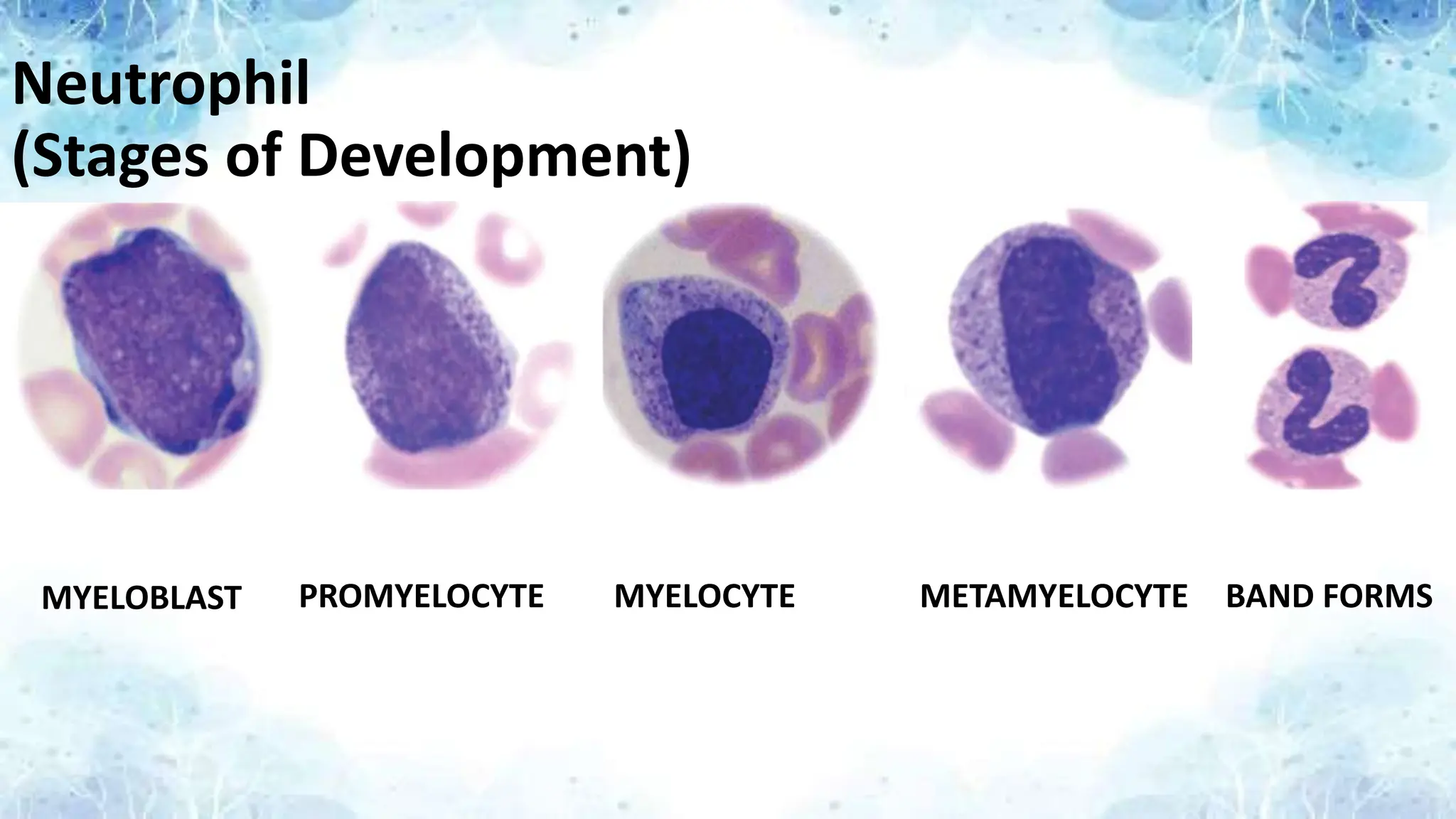
Neutrophil
• 40 to80 percent of total WBC
count(2.0-7.0 x109/1)
• Diameter - 13 μm
• Segmented Nucleus and pink/orange
cytoplasm with fine granulation(0.2-
0.3μm)
• Lobes -2-5
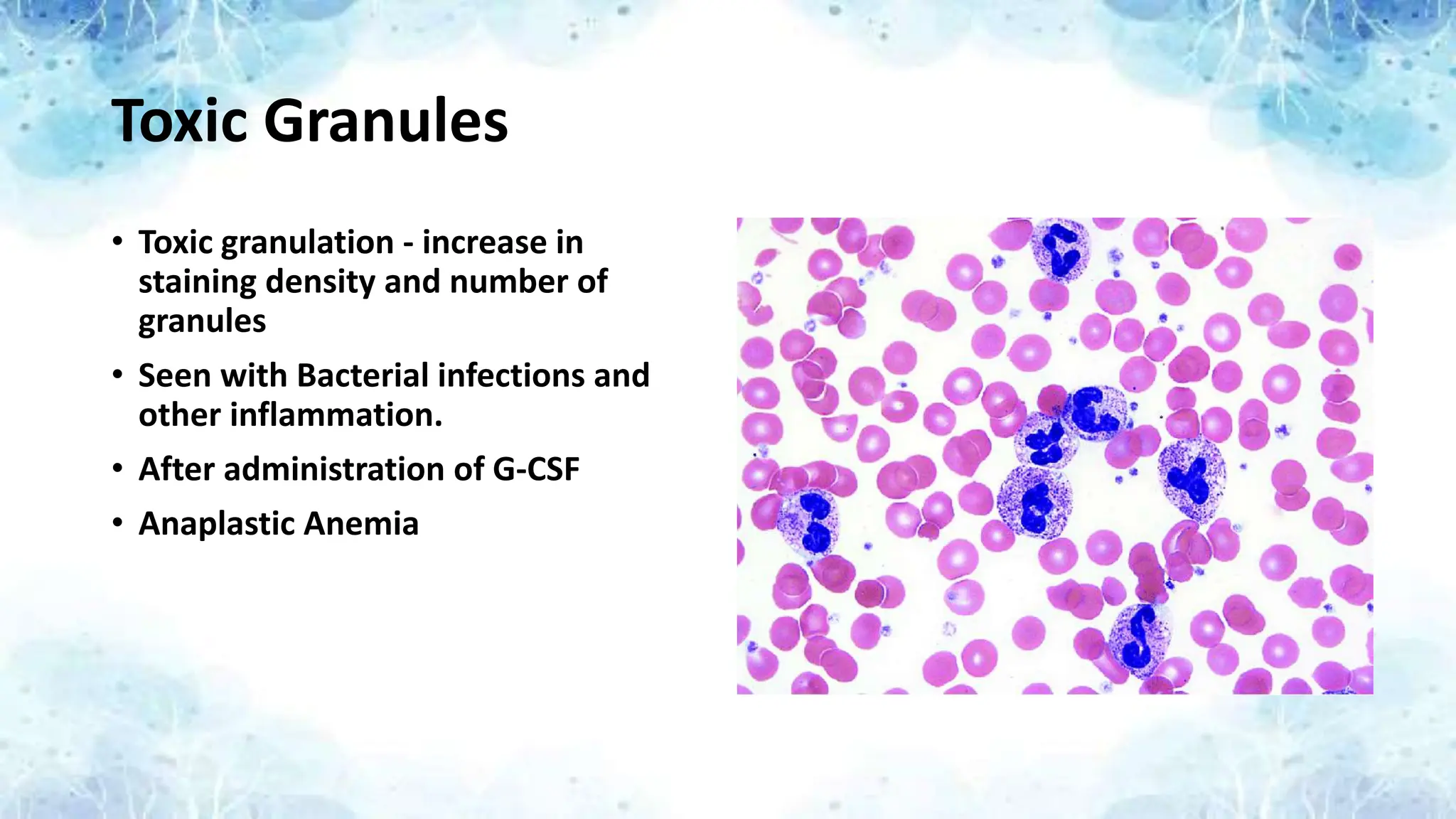
Toxic Granules
• Toxicgranulation - increase in
staining density and number of
granules
• Seen with Bacterial infections and
other inflammation.
• After administration of G-CSF
• Anaplastic Anemia
42.
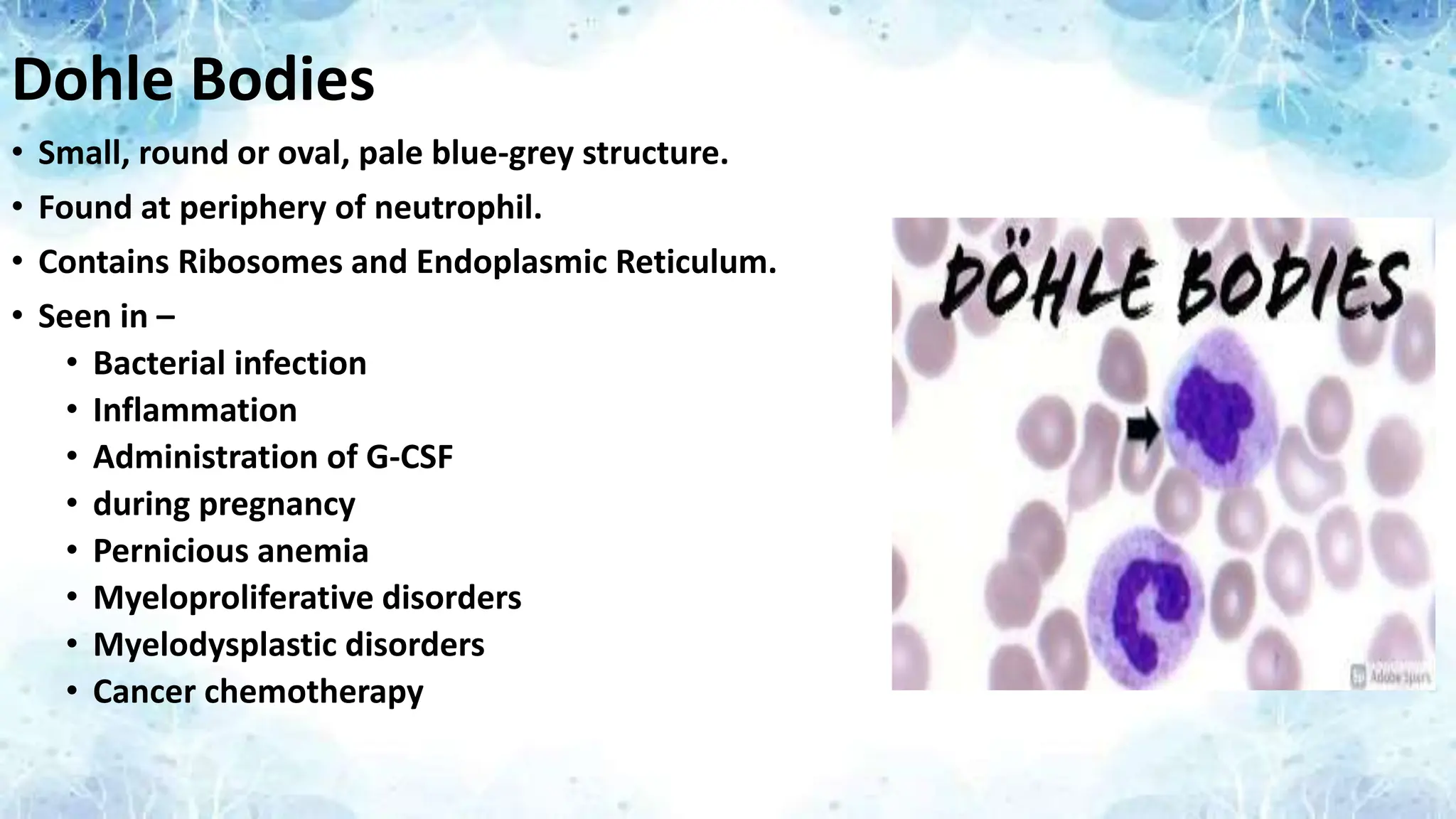
Dohle Bodies
• Small,round or oval, pale blue-grey structure.
• Found at periphery of neutrophil.
• Contains Ribosomes and Endoplasmic Reticulum.
• Seen in –
• Bacterial infection
• Inflammation
• Administration of G-CSF
• during pregnancy
• Pernicious anemia
• Myeloproliferative disorders
• Myelodysplastic disorders
• Cancer chemotherapy
43.
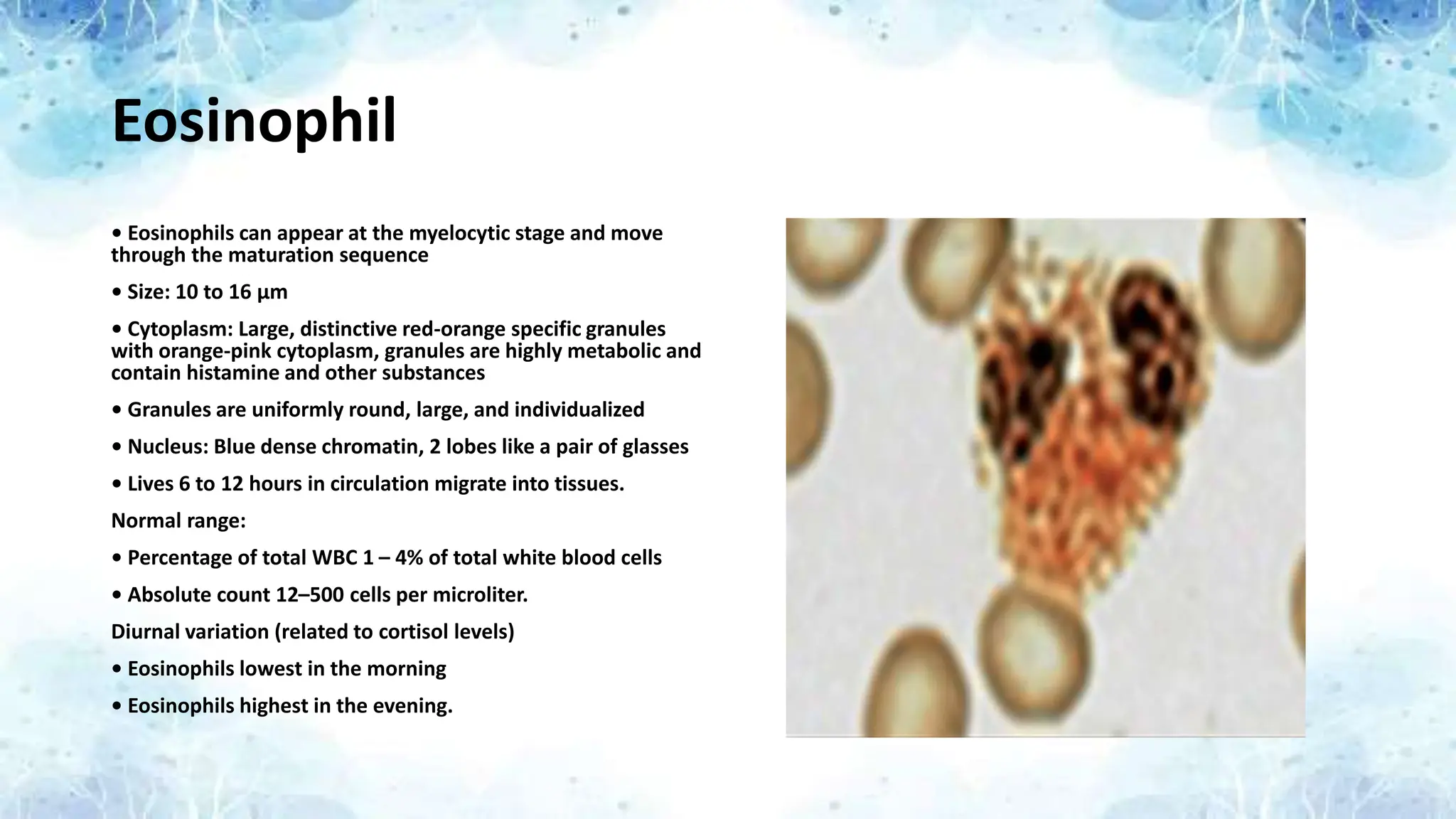
Eosinophil
• Eosinophils canappear at the myelocytic stage and move
through the maturation sequence
• Size: 10 to 16 μm
• Cytoplasm: Large, distinctive red-orange specific granules
with orange-pink cytoplasm, granules are highly metabolic and
contain histamine and other substances
• Granules are uniformly round, large, and individualized
• Nucleus: Blue dense chromatin, 2 lobes like a pair of glasses
• Lives 6 to 12 hours in circulation migrate into tissues.
Normal range:
• Percentage of total WBC 1 – 4% of total white blood cells
• Absolute count 12–500 cells per microliter.
Diurnal variation (related to cortisol levels)
• Eosinophils lowest in the morning
• Eosinophils highest in the evening.
44.
Causes of Eosinophiliaand Eosinopenia
Eosinophilia
Mild (700–1500 per microliter)
• Allergic rhinitis, extrinsic asthma, mild drug reaction, long-
term dialysis, immunodeficiency
Moderate (1500–5000 per microliter)
• Parasitic disease, intrinsic asthma, pulmonary eosinophilia
syndrome
Marked (> 5000 per microliter)
• Trichinella, hookworm, Toxocara canis, eosinophilic
leukemia, severe drug reaction.
OTHER CAUSES
• Drug induced eosinophilia
• Severe, long-standing rheumatoid arthritis
• Psoriasis
• Crohn’s disease, ulcerative colitis
• Systemic lupus erythematosus
• Malignant disease
• Implies metastatic disease—Poor prognosis
• Hypopituitarism (decreased steroids)
• No identifiable causes— Hyper-eosinophilic syndromes
Eosinopenia
• Usually related to increased circulating steroids
• Aplastic Anemia.
• Cushing’s syndrome
• Drugs
• ACTH, epinephrine, thyroxine, exogenous steroids
• Acute bacterial infection
45.
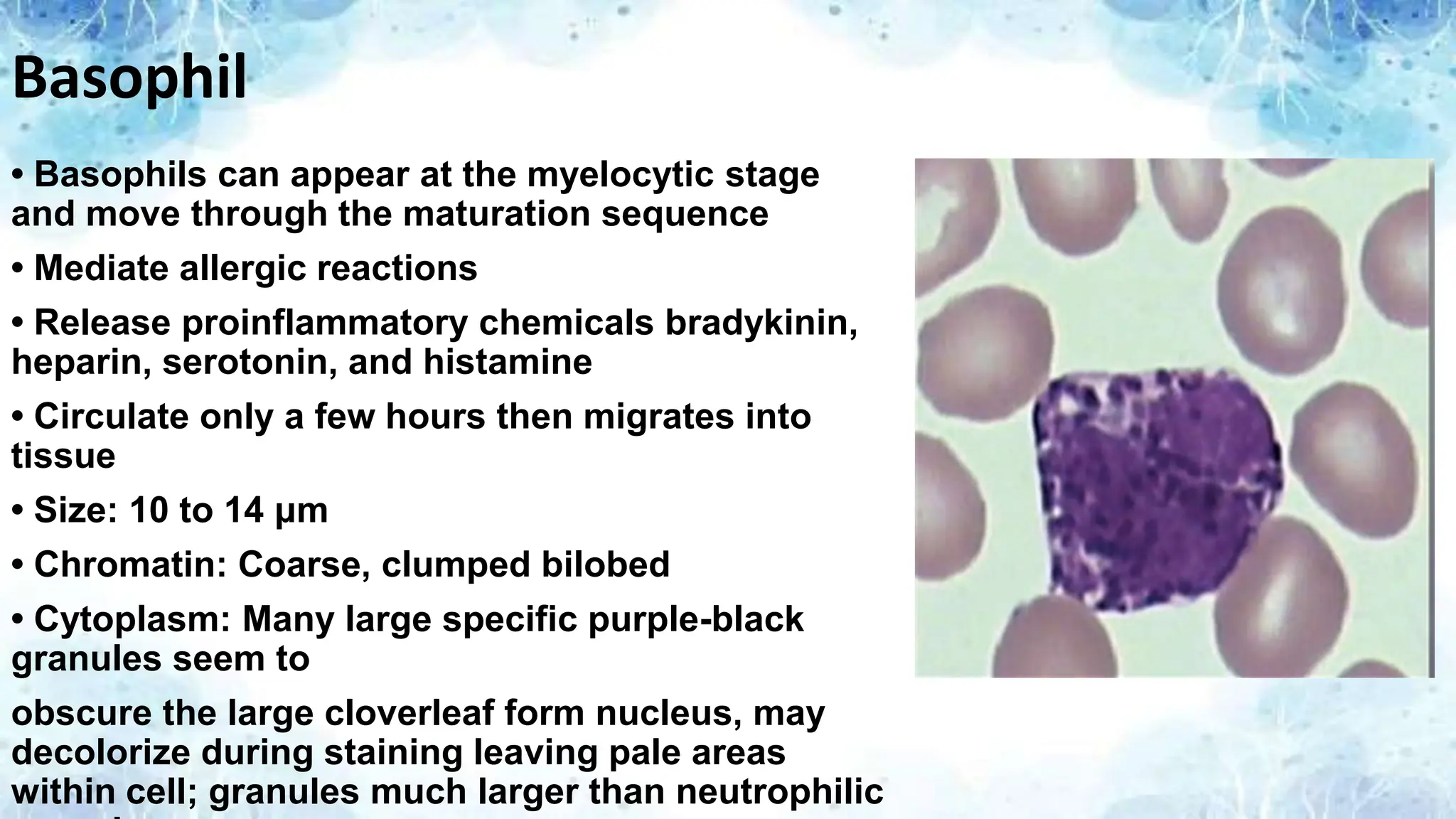
Basophil
• Basophils canappear at the myelocytic stage
and move through the maturation sequence
• Mediate allergic reactions
• Release proinflammatory chemicals bradykinin,
heparin, serotonin, and histamine
• Circulate only a few hours then migrates into
tissue
• Size: 10 to 14 μm
• Chromatin: Coarse, clumped bilobed
• Cytoplasm: Many large specific purple-black
granules seem to
obscure the large cloverleaf form nucleus, may
decolorize during staining leaving pale areas
within cell; granules much larger than neutrophilic
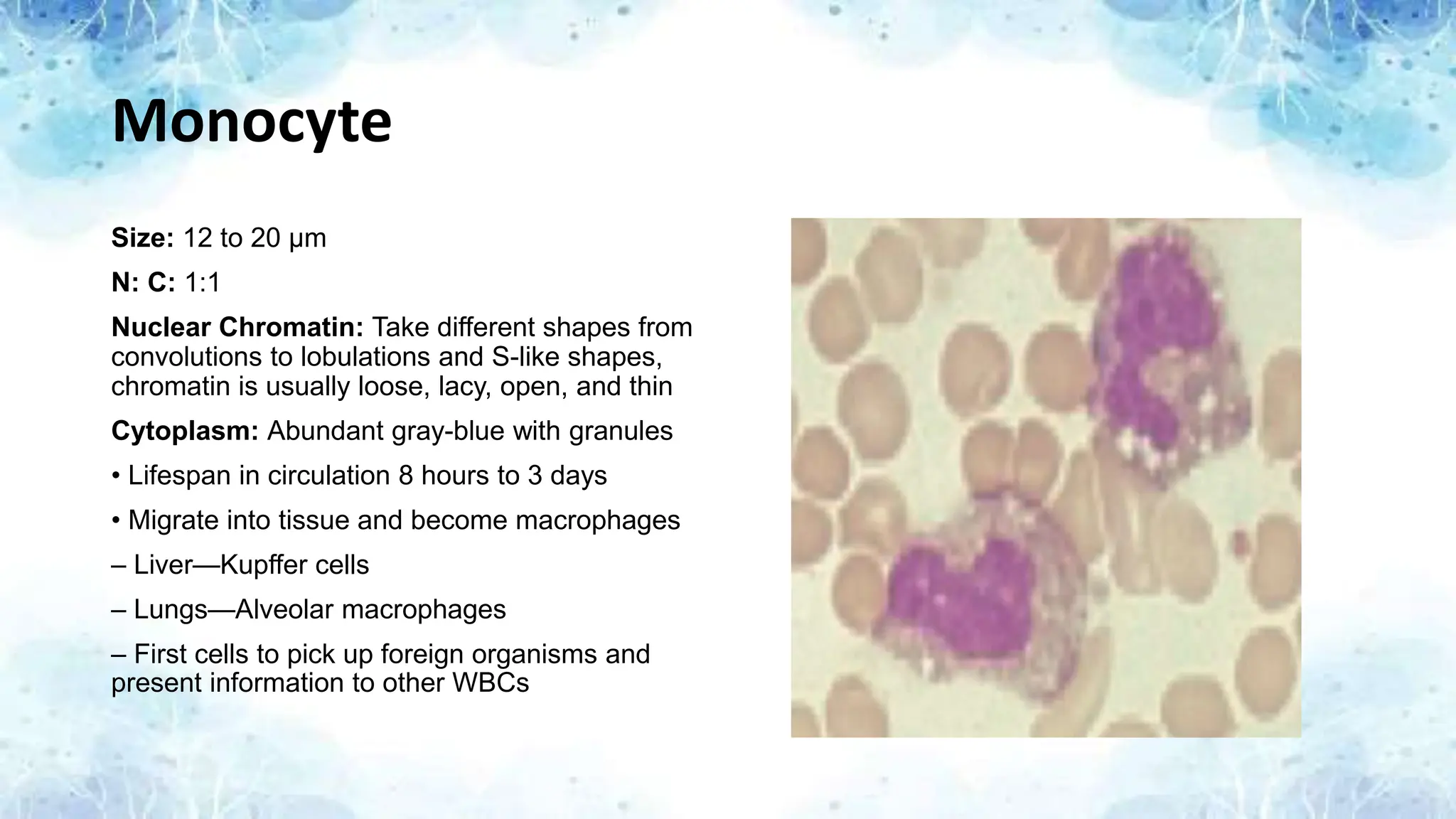
Monocyte
Size: 12 to20 μm
N: C: 1:1
Nuclear Chromatin: Take different shapes from
convolutions to lobulations and S-like shapes,
chromatin is usually loose, lacy, open, and thin
Cytoplasm: Abundant gray-blue with granules
• Lifespan in circulation 8 hours to 3 days
• Migrate into tissue and become macrophages
– Liver—Kupffer cells
– Lungs—Alveolar macrophages
– First cells to pick up foreign organisms and
present information to other WBCs
50.
Causes of Monocytosisand Monocytopenia
Monocytosis
Monocyte levels > than 700 /mcl or > than 12% of WBCs.
Usual causes:
• Viral infections
• Tuberculosis
• Subacute bacterial endocarditis
• Collagen diseases
• Chronic inflammation
• Stress response
• Hyperadrenocorticism
• Infectious mononucleosis
• Sarcoidosis
• Concomitant with neutrophilia
• Autoimmune conditions
• Crohn’s disease
• Rheumatoid disease
• Systemic lupus erythematosus
• Ulcerative colitis.
Monocytopenia
Very uncommon by itself.
Usual causes:
• Hairy cell leukemia
• Aplastic anemia
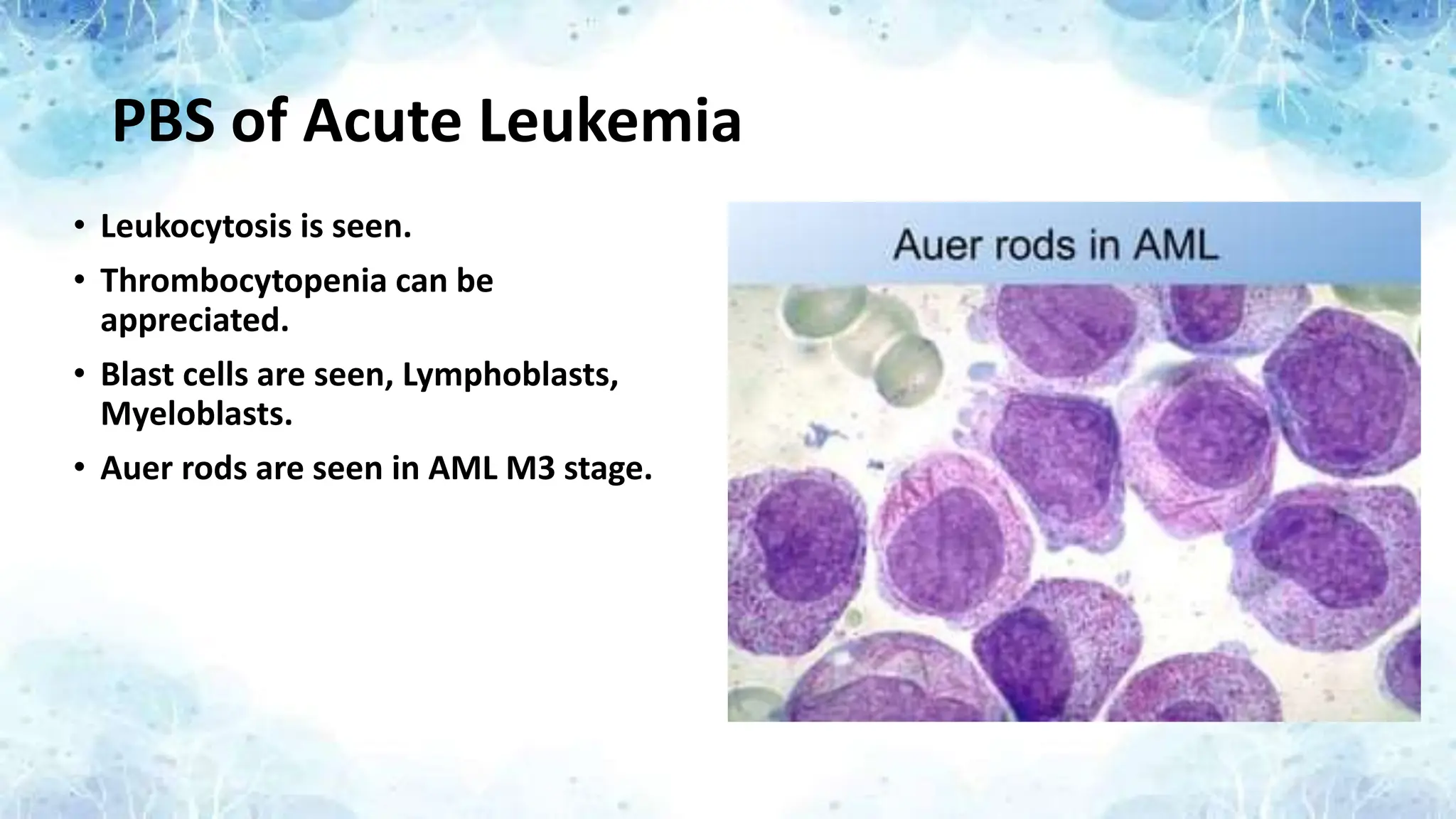
PBS of AcuteLeukemia
• Leukocytosis is seen.
• Thrombocytopenia can be
appreciated.
• Blast cells are seen, Lymphoblasts,
Myeloblasts.
• Auer rods are seen in AML M3 stage.
53.
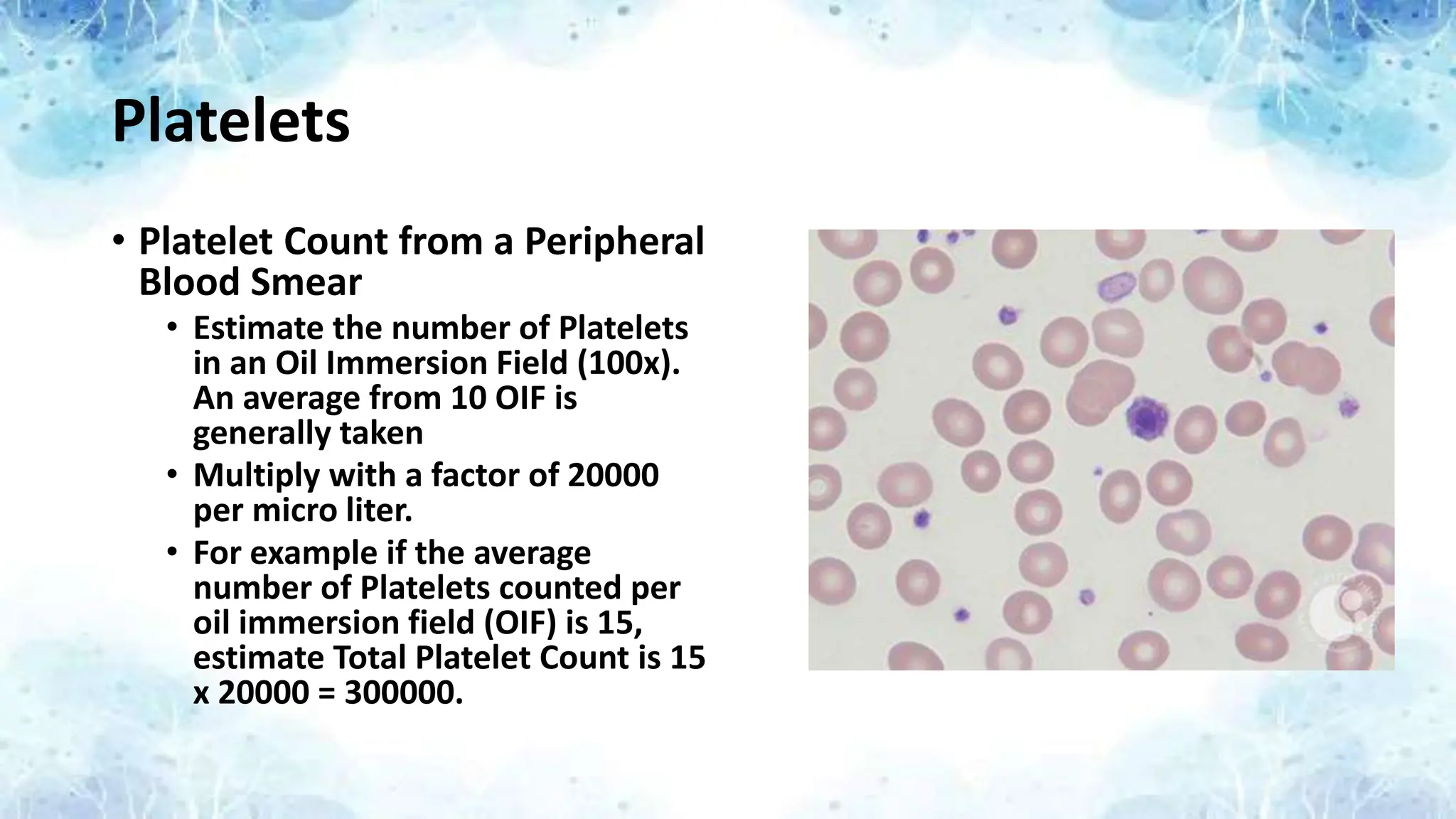
Platelets
• Platelet Countfrom a Peripheral
Blood Smear
• Estimate the number of Platelets
in an Oil Immersion Field (100x).
An average from 10 OIF is
generally taken
• Multiply with a factor of 20000
per micro liter.
• For example if the average
number of Platelets counted per
oil immersion field (OIF) is 15,
estimate Total Platelet Count is 15
x 20000 = 300000.
54.
Causes of Thrombocytopenia(Decreased
Platelet Production)
• Amegakaryocytic thrombocytopenia
• Aplastic anemia
• Myelodysplastic syndrome (MDS)
• Bone marrow hypoplasia due to—
– Chemotherapy
– Radiation
– Toxins
– Immune.
• Myelophthisic Anemia
• Myeloproliferative Disorders
• Selective marrow suppression of platelet production due to—
– Drugs
– Infections
– Ethanol.
• Ineffective thrombopoiesis due to—
– Folate or B12 deficiency.
• Hereditary disorders
– Wiskott-Aldrich syndrome.
55.
Causes of Thrombocytopenia(Increased
Platelet Destruction)
Immune mediated
• Idiopathic/immune thrombocytopenia (ITP).
• Systemic lupus erythematosus
• Lymphoproliferative disorders
• Drugs including heparin induced
• Infections including HIV related
• Post-transfusion purpura
Nonimmune mechanisms
• Severe bleeding
• Disseminated intravascular coagulation (DIC)
• Abnormalities in small vessels
• Vasculitis
• von Willebrand disease (vWD)
• Thrombotic thrombocytopenic purpura
• Hemolytic uremic syndrome.
56.
Platelet Morphology
• Normalplatelets are about 1–3 μm in diameter, blue-gray, and contain fine,
purple to pink granules that may be diffuse or concentrated in the center of the
cells.
• Normally the ratio of red cells to platelets is about 10–40:1.
• Approximately 7–20 platelets are present in each oil immersion field.
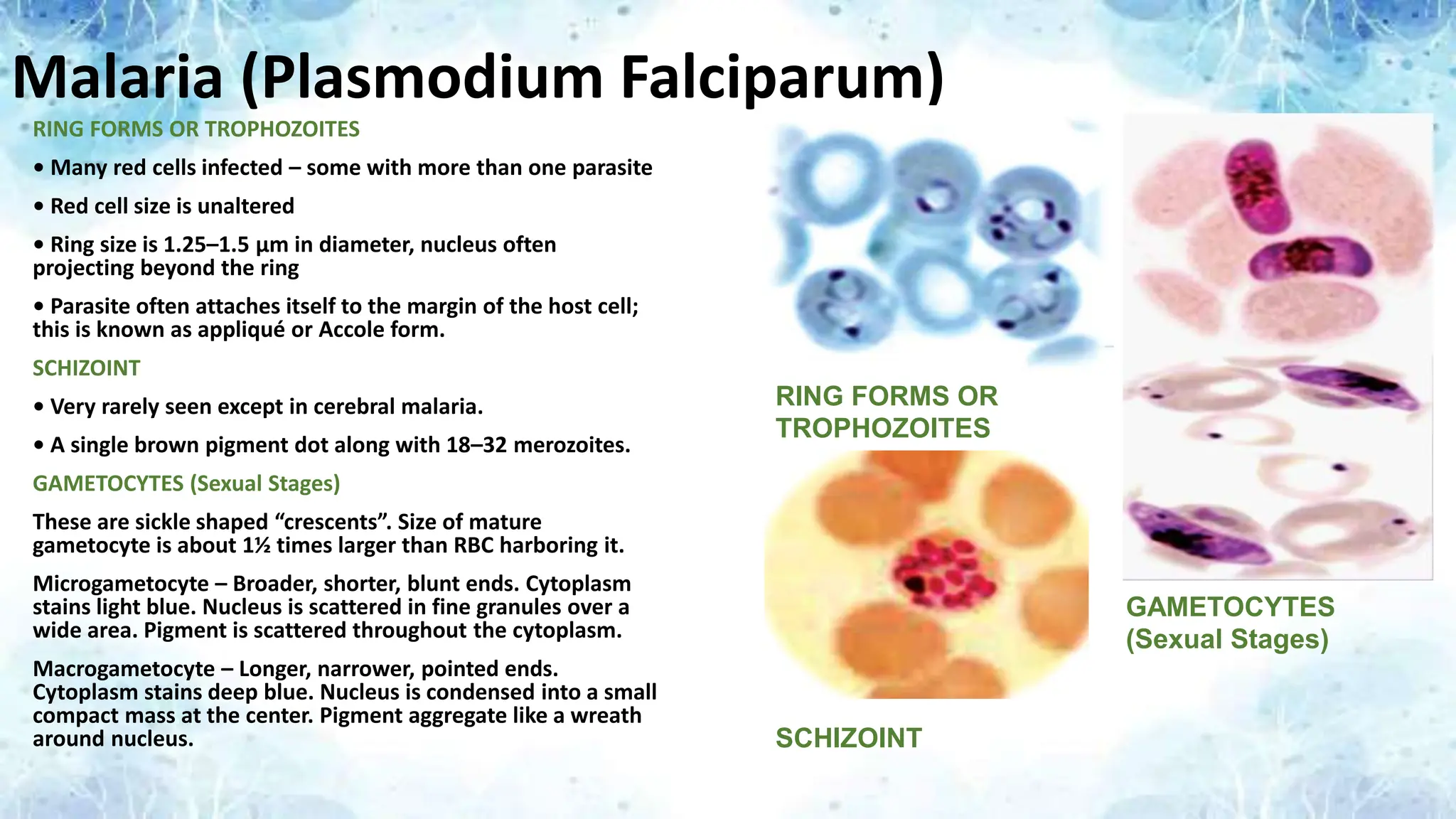
Malaria (Plasmodium Falciparum)
RINGFORMS OR TROPHOZOITES
• Many red cells infected – some with more than one parasite
• Red cell size is unaltered
• Ring size is 1.25–1.5 μm in diameter, nucleus often
projecting beyond the ring
• Parasite often attaches itself to the margin of the host cell;
this is known as appliqué or Accole form.
SCHIZOINT
• Very rarely seen except in cerebral malaria.
• A single brown pigment dot along with 18–32 merozoites.
GAMETOCYTES (Sexual Stages)
These are sickle shaped “crescents”. Size of mature
gametocyte is about 1½ times larger than RBC harboring it.
Microgametocyte – Broader, shorter, blunt ends. Cytoplasm
stains light blue. Nucleus is scattered in fine granules over a
wide area. Pigment is scattered throughout the cytoplasm.
Macrogametocyte – Longer, narrower, pointed ends.
Cytoplasm stains deep blue. Nucleus is condensed into a small
compact mass at the center. Pigment aggregate like a wreath
around nucleus.
RING FORMS OR
TROPHOZOITES
SCHIZOINT
GAMETOCYTES
(Sexual Stages)
59.
Malaria (Plasmodium Vivax)
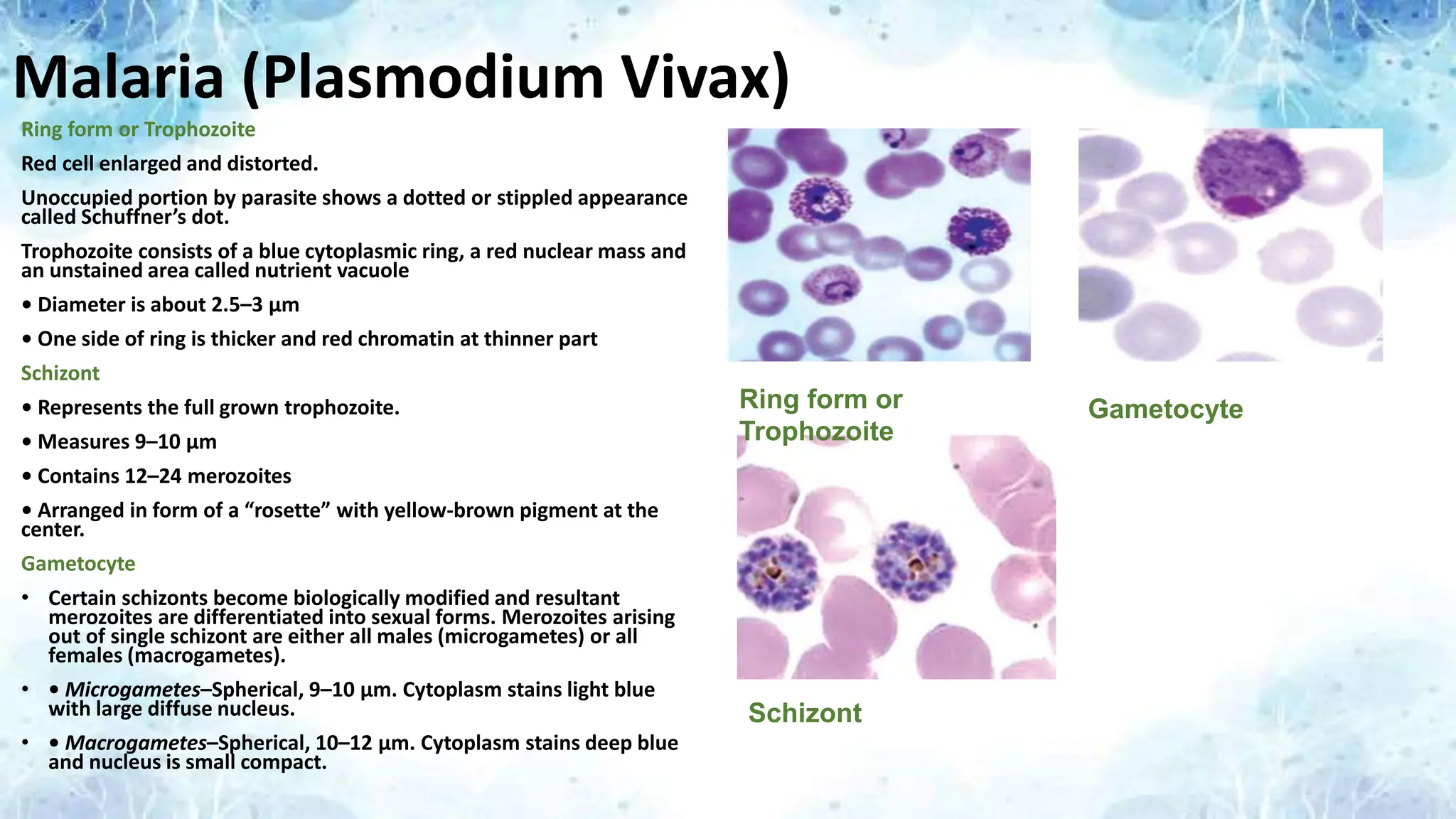
Ringform or Trophozoite
Red cell enlarged and distorted.
Unoccupied portion by parasite shows a dotted or stippled appearance
called Schuffner’s dot.
Trophozoite consists of a blue cytoplasmic ring, a red nuclear mass and
an unstained area called nutrient vacuole
• Diameter is about 2.5–3 μm
• One side of ring is thicker and red chromatin at thinner part
Schizont
• Represents the full grown trophozoite.
• Measures 9–10 μm
• Contains 12–24 merozoites
• Arranged in form of a “rosette” with yellow-brown pigment at the
center.
Gametocyte
• Certain schizonts become biologically modified and resultant
merozoites are differentiated into sexual forms. Merozoites arising
out of single schizont are either all males (microgametes) or all
females (macrogametes).
• • Microgametes–Spherical, 9–10 μm. Cytoplasm stains light blue
with large diffuse nucleus.
• • Macrogametes–Spherical, 10–12 μm. Cytoplasm stains deep blue
and nucleus is small compact.
Ring form or
Trophozoite
Schizont
Gametocyte
60.
Filariasis
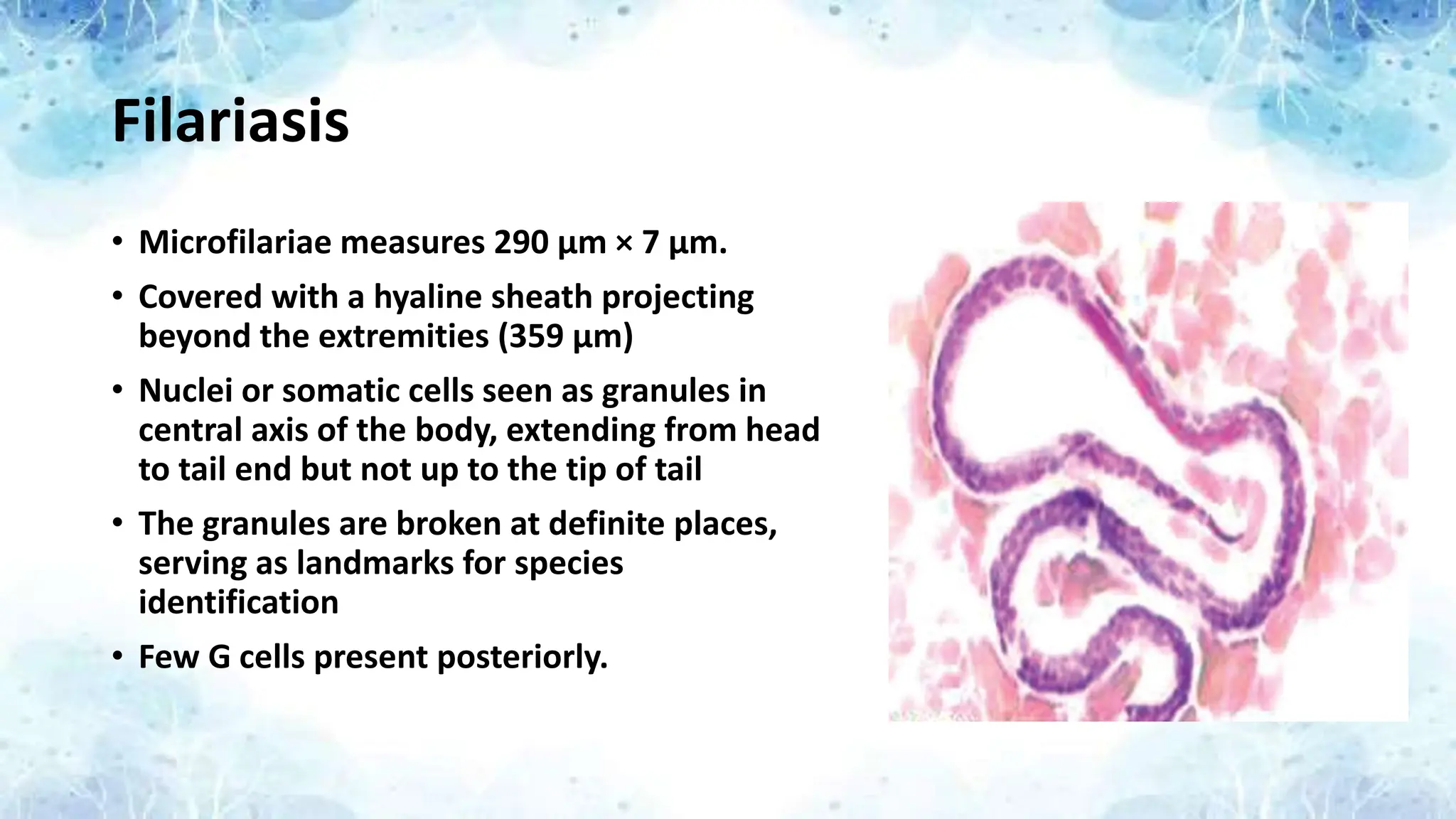
• Microfilariae measures290 μm × 7 μm.
• Covered with a hyaline sheath projecting
beyond the extremities (359 μm)
• Nuclei or somatic cells seen as granules in
central axis of the body, extending from head
to tail end but not up to the tip of tail
• The granules are broken at definite places,
serving as landmarks for species
identification
• Few G cells present posteriorly.
61.
Leishmaniasis
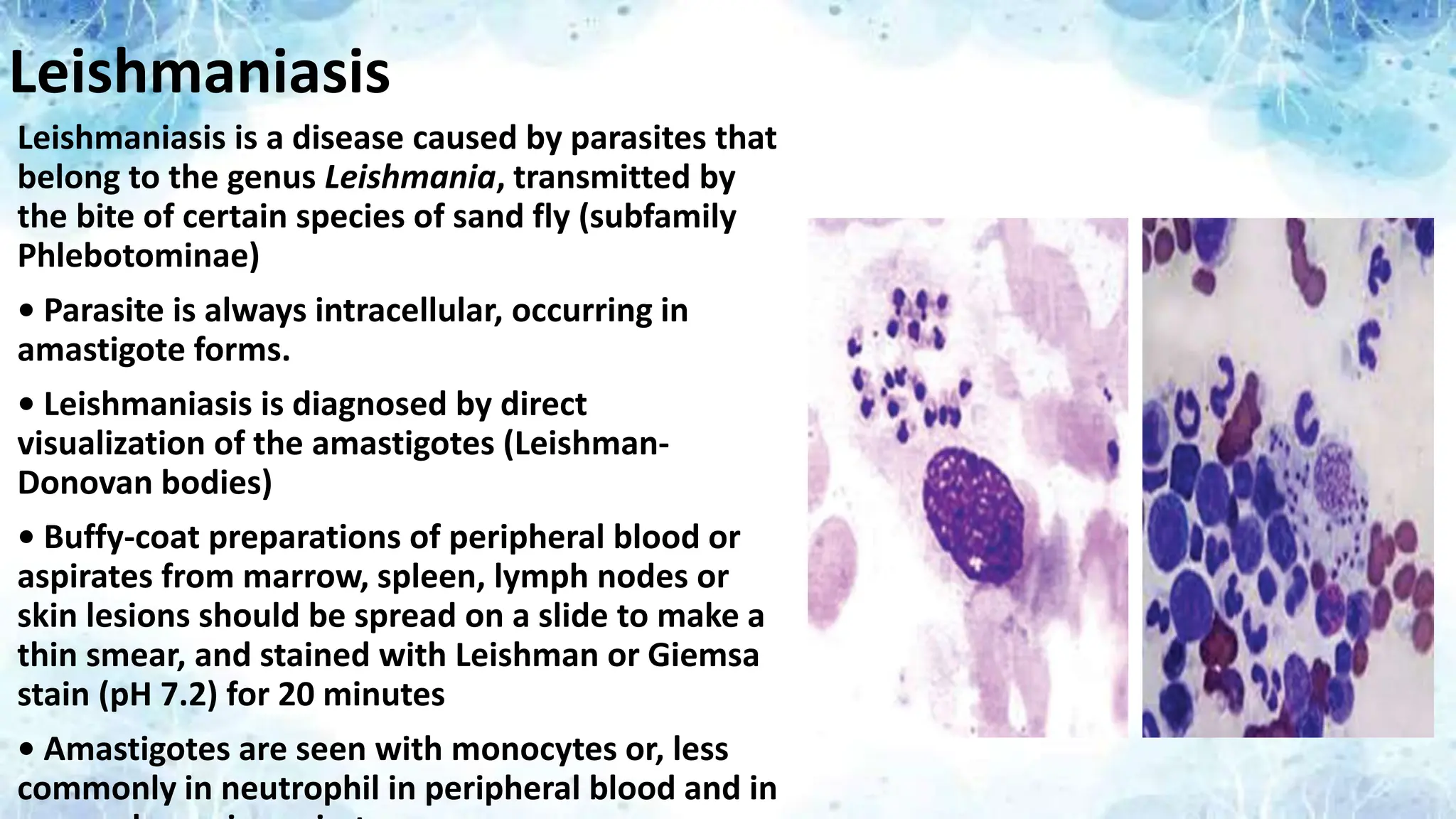
Leishmaniasis is adisease caused by parasites that
belong to the genus Leishmania, transmitted by
the bite of certain species of sand fly (subfamily
Phlebotominae)
• Parasite is always intracellular, occurring in
amastigote forms.
• Leishmaniasis is diagnosed by direct
visualization of the amastigotes (Leishman-
Donovan bodies)
• Buffy-coat preparations of peripheral blood or
aspirates from marrow, spleen, lymph nodes or
skin lesions should be spread on a slide to make a
thin smear, and stained with Leishman or Giemsa
stain (pH 7.2) for 20 minutes
• Amastigotes are seen with monocytes or, less
commonly in neutrophil in peripheral blood and in
62.
Babesiosis
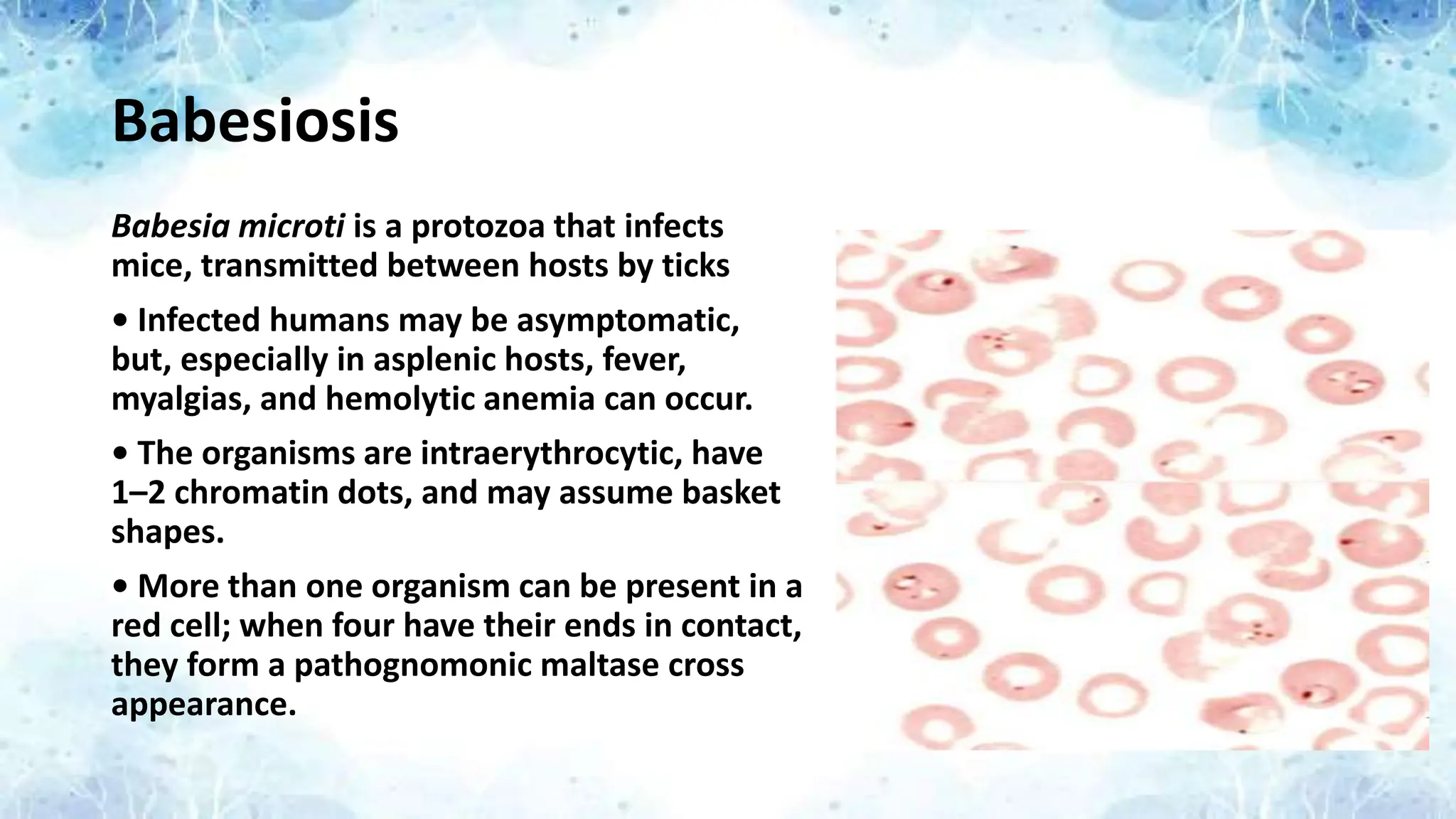
Babesia microti isa protozoa that infects
mice, transmitted between hosts by ticks
• Infected humans may be asymptomatic,
but, especially in asplenic hosts, fever,
myalgias, and hemolytic anemia can occur.
• The organisms are intraerythrocytic, have
1–2 chromatin dots, and may assume basket
shapes.
• More than one organism can be present in a
red cell; when four have their ends in contact,
they form a pathognomonic maltase cross
appearance.
63.
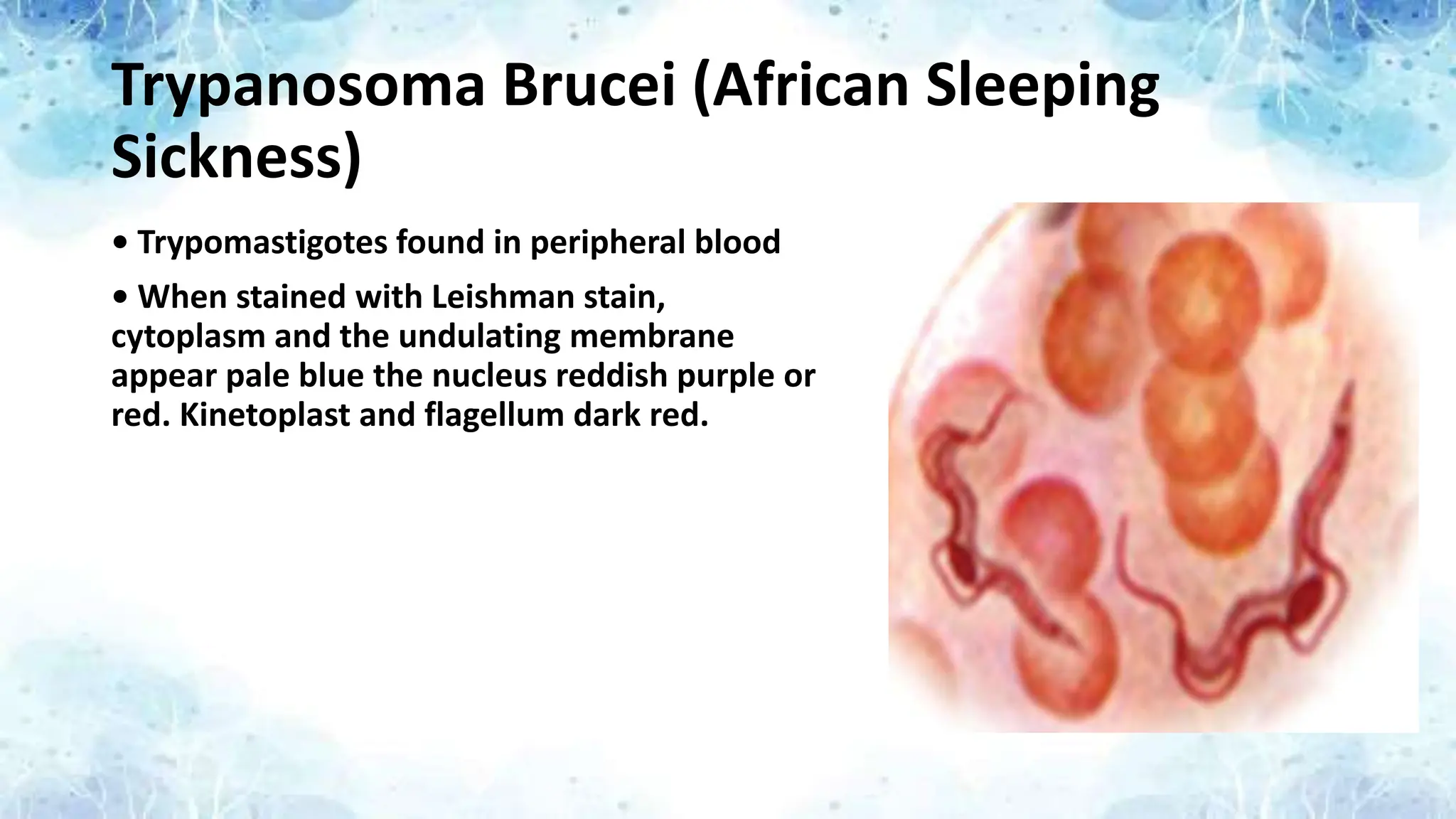
Trypanosoma Brucei (AfricanSleeping
Sickness)
• Trypomastigotes found in peripheral blood
• When stained with Leishman stain,
cytoplasm and the undulating membrane
appear pale blue the nucleus reddish purple or
red. Kinetoplast and flagellum dark red.
64.
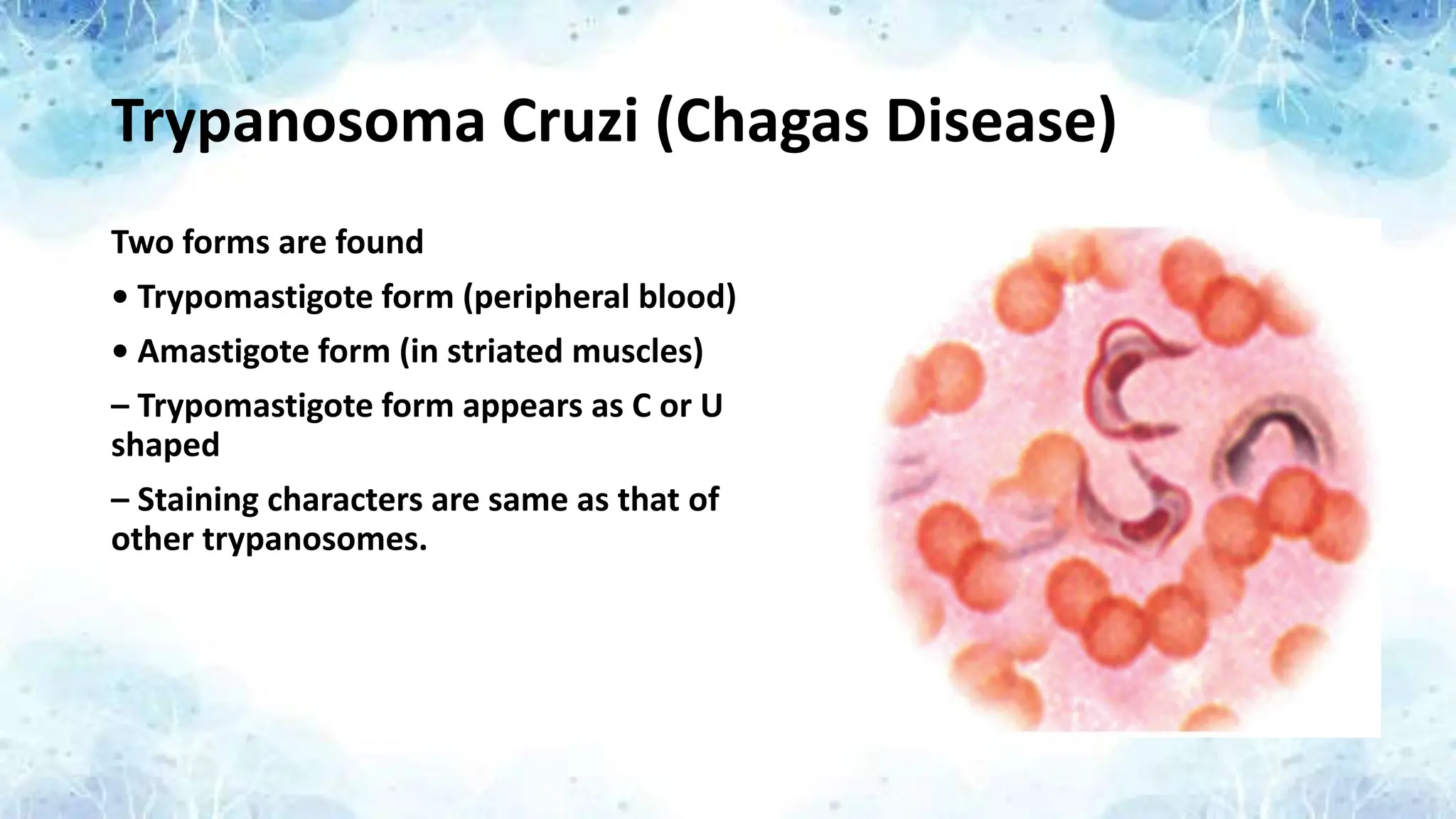
Trypanosoma Cruzi (ChagasDisease)
Two forms are found
• Trypomastigote form (peripheral blood)
• Amastigote form (in striated muscles)
– Trypomastigote form appears as C or U
shaped
– Staining characters are same as that of
other trypanosomes.
65.
Significance of PeripheralBlood Smear
• It provides rapid, reliable access to information about a variety of
hematologic disorders.
• Examination of the peripheral blood smear is an inexpensive but
powerful diagnostic tool in both children and adults.
• The smear offers a window into the functional status of the bone
marrow.
• Review of the smear is an important adjunct to other clinical data;
in some cases, the peripheral smear alone is sufficient to establish a
diagnosis.
66.
References
• Robbins AndCotran – Pathologic Basis of Disease
• ABC of CBC – DP Lokwani
• Essentials of Hematology – Shirish M Kawthalkar