Downloaded 182 times
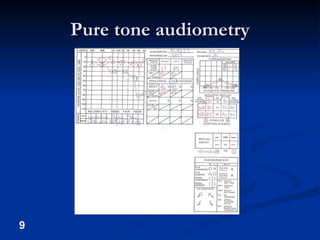


This document discusses the assessment of both peripheral and central auditory function. It describes tests used to evaluate the peripheral auditory system including pure tone audiometry, speech audiometry, and otoacoustic emissions. It also discusses tests of central auditory processing such as the staggered spondaic word test, speech-in-noise test, and masking level difference test. The document emphasizes the importance of a multidisciplinary approach involving otologists, speech pathologists, and audiologists in evaluating both peripheral hearing and central auditory processing.








































![Introduction to hearing implairment & cochlear implantation]](https://cdn.slidesharecdn.com/ss_thumbnails/introductiontohearingimplairmentcochlearimplantation-161111054000-thumbnail.jpg?width=640&height=640&fit=bounds)














![Mai EchoG and OAEs ENT [Recovered].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/maiechogandoaesentrecovered-230503021828-debb4756-thumbnail.jpg?width=640&height=640&fit=bounds)






























