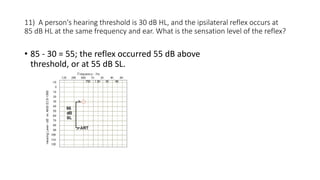
- A cochlear loss typically results in acoustic reflexes present at normal hearing levels (below 100 dB HL), but at reduced sensation levels (less than 65 dB above the hearing threshold). Significant reflex decay is not expected.
- A conductive loss usually results in absent ipsilateral acoustic reflexes in the ear with the loss. A contralateral reflex may be present if the loss is unilateral and not severe. Any reflex found would be at a normal sensation level but a higher hearing level due to the elevated threshold.
- A retrocochlear loss may result in absent reflexes or ones present at elevated hearing and sensation levels. Early on a reflex may be present but reflex decay would be found.





































![Introduction to hearing implairment & cochlear implantation]](https://cdn.slidesharecdn.com/ss_thumbnails/introductiontohearingimplairmentcochlearimplantation-161111054000-thumbnail.jpg?width=640&height=640&fit=bounds)








































