What is anAudiological Evaluation?
An audiological evaluation is a series of tests called as (Audiological test
battery ) use to determine the type, degree and configuration of hearing
loss. The tests often provide insights on what the causes of hearing loss. And
we can use the information and results to develop a treatment plan that will
be most effective to each diagnosis
An audiological evaluation may be performed by an audiologist or
Audilovestibular specialist
Audiological evaluation best performed according to the age of
patients ,social and medical conditions of patients availability of equipment's
, & experience of medical & technical staff
3.
Terminology
Hearing lossis a medical term that refers to degree of patients hearing difficulty
measured by dBHL
Hearing impaired is public term used to describe people with any degree of
hearing loss, from mild to profound, including those who are deaf and those who
are hard of hearing.
Hearing disability refers to hearing loss greater than (35dB) in the better
hearing ear
Frequency sometimes referred to as pitch, is the number of times per second
that a sound pressure wave repeats itself (F = cycles / time ) Hz
http://www.hearingloss.org/
4.
Sound intensity(loudness ) is defined as the sound power per unit area . whereas
amplitude is the distance between the resting position and the crest of a wave. Unite
of intensity in general is the but sound intensity use the (deciBel) dB HL or SPL
Audiological Assessments
Subjective tests
Subjective audiometry tests
depending on the subjective
responses from the patients to
various sound stimuli. That
make the patient have a roll in
the test results
Pure tone audiometry
Speech Audiometry
Objective
Objective audiometry tests measures the
electrical activity in the auditory pathway. It
does not require a patient to participate.
And haven't rol in the test results
Impedance Audiometry (Tympanometry ,
acoustics reflexes ,reflex decay & ETF )
OAE (TE OAE ,DP OAE )
ABR / ASSR
EchoG
7.
Pure Tone Audiometry
Subjective test measure the acuity of hearing threshold of an individual
by instrument known as the audiometer.
Hearing threshold : is the lowest level of sound where the patient can hear
in 50% of times For each specific frequency .
1. To know whether the subject has any definitive H.L.
2. To know the types of H.L( conductive , mixed or
sensorineural ( cochlear or retro-cochlear ) by use special
tests ( SISI ,ABLB ,Stenger )
3.To determine The degree of hearing dysfunctions (mild –
moderate – sever or profound )
4. To show the configuration of hearing loss curve
The aims of PTA
8.
Diagnostic standard audiometer
2channals ( masking )
AC Freg :125 Hz - 12KHz
Intensity -10 -120 dBHL
BC : -10 -80 dBHL
screening audiometer
AC , one intensity ,3
frequencies ,pass or failed
Computer based audiometer
AUDIOMETER TYPES
Play audiometer/VRA
9.
Tranceducers & basiccompenants
Supra-aural:TDH-39
Circumaural:HDA200
bone oscillator B71 . B81
Inserted:ER
Loudspeakers
Diagnostic PTA
AC Conduction
BC Conduction Free field test & S. Aud
.
Freq selector dial
Intensity selector dial
Tone presentation switch
Output selector
Earphone AC, L&R ear
Masking on /off
Microphone
IAA 55dB IAA 0dB
IAA 45dB
IAA 40dB
10.
Sound attenuatingroom
Single or double walled ,4 inch thick
Inside wall covered with sound absorbed material ,
small holes to absorb sound to decrease
reflection .
Patient positioned :-
45 -90 degree :
away from the examiner for adult
And away from the speaker in case of visually
reinforcement Audiometry in children .
Face the speaker :
patient with hearing aid To ensure that the sound is
directed to the microphone of the hearing aid
The test Environment
11.
Calibration shouldinvolves calibration of audiometer, earphones and bone
vibrators , Can be performed using human volunteers and artificial ears
Malingerer’s should be tested only by an audiologist
Short brief history & rapid local examination
Otoscopy & Tympanometry should be done prior to audiometry
Test procedure should be fully explained to the patient
Glasses / ear rings should be removed
start with the better ear or the right ear
Red headphone is placed over right ear
BiL AC before BiL BC
Before testing
-:
06/16/2025 13
Hearing LevelHL ??
Human hearing varies according to
the frequency of the sound
At 1000 Hz the weakest sound a
normal-hearing person can hear is
7.0 dB SPL 1000 Hz
At 4000 Hz the normal threshold is
12.0 dB SPL becomes 0 dB HL at 0
dB HL at 4000 Hz
The relationship between HL and
SPL is defined by ANSI S3.6-1996.
Each of these SPLs becomes 0 dB
HL at the test frequency.
Reference Equivalent Threshold Sound Pressure Levels
0
5
10
15
20
25
30
35
40
45
50
125 250 500 750 1000 1500 2000 3000 4000 6000 8000
Frequency (Hz)
S
o
u
n
d
P
re
s
s
u
re
L
e
v
e
l
(d
B
)
dBSPL
dBHL
SPL= (HL) X (RE SPL) / 10 AT 1000Hz
SPL= 50db HL X 7/10
=
SPL = 350 / 10 = 35 dBSPL
HL = SPL / (RE spl ) X 10 AT 500Hz
HL = 40 / 15 X 1O
HL = 2.6 X 10 = 26 dBHL
?
?
14.
HOW READING AUDIOGRAM?
1
-
Identification
2
-
PTA notes ( IAA , A/B gap
indication of masking
3
-
Response Consistency
(good ,intermediat ,poor )
4
-
Validity of test(reliable or
questionable )
5
-
PT Average
,
6
-
Degree of hearing loss
7
-
Type of hearing loss
.
8
-
Configuration of PTA
9
-
Report or comments
.
Steps of PTA reading
-:
Direction ,degree ,type , configuration , notes ,recommendation
15.
2- PTA notes( IAA , A/B gap ) indication of masking
Masked
Unmasked
Lt HT = 65 dB
Lt HT = 50 dB
SNHL
Mixed HL
16.
3,4- Response consistency& validity of the test:-
Poor: many false negative & false positive responses.
Intermediate : moderate amounts of false negative & positive responses.
Good : no or minimum amounts
False +ve : no stimulus , response present.
False –ve : suprathreshold stimulus ,no response
validity of the test ( reliable results or questionable )
Subsequent test results should vary not more than 5dB .
17.
5dB 10
dB 500Hz
20
dB15
dB 1kHz
25
dB 20dB 2
KH
40
dB 30
dB 4
KH
PTA AVG (500 – 4000Hz) in dB
Best binaural to
correlate with FFT
or SDT
LT-HT(dBHL) R-HT (dBHL)
13 13 15 Three freq
23 22 18 Four freq
17
06/16/2025
Freq. Rt-Ear Lt-ear
5-PT Average ?
18.
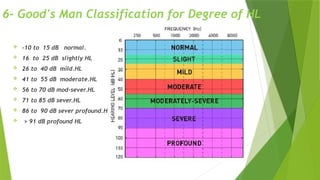
6- Good's ManClassification for Degree of HL
-10 to 15 dB normal.
16 to 25 dB slightly HL
26 to 40 dB mild.HL
41 to 55 dB moderate.HL
56 to 70 dB mod-sever.HL
71 to 85 dB sever.HL
86 to 90 dB sever profound.HL
> 91 dB profound HL
19.
7-Types of HearingLoss
Conductive Loss ( Abnormal AC , Normal BC ,ABG > 10dB )
Sensorineural Loss ( Abnormal AC , Abnormal BC ,ABG <10dB )
(Sensory or Neural ? )
Mixed Hearing Loss ( Abnormal AC , Abormal BC ,ABG > 10dB )
Normal for speech frequncies (Normal AC& BC For speech Feq. Only )
Normal with Conductive element. ( Normal AC , Normal BC ,ABG > 10dB )
20.
HT=5dB (Normal )HT=18dB (Normal
with cond.element )
HT=70dB (Mixed HL) HT=65dB (SNHL)
A/B gap > 10 dB
HT=40dB
(Conductive HL)
HT=15dB (Normal for
speech freq.)
21.
8-Configuration of PTA
Flat <5dB average difference per octave
Gradually sloping 6-10dB rise or fall per octave
Sharply sloping 11-15dB rise or fall per octave
Abruptly sloping ≥16dB rise or fall per octave
Rising Better hearing at the higher frequencies
Trough or saucer ≥20dB more loss at middle frequencies than at 250 and
8000Hz
Notch Sharply poorer at one frequency, with recovery at adjacent frequencies
Limitation of PTA
Subjective test
Improper masking
Faulty placements of headphones and vibrator
Occlusion effect during BC
Noisy environment
Improper calibration of audiometers
Improper examiner
24.
24
Speech Audiometry
Comprehension Understandingthe meaning
identification Can say what the word is
Discrimination Can tell the difference between words
Detection Can say speech is present
Define as the measurement of patient's ability to hear and understand the
speech
.
It is complementary to pure tone audiometry ; which only gives an
indication of absolute perceptual thresholds of tonal sound (peripheral
function), whereas speech audiometry determines speech intelligibility
and discrimination .
25.
Speech Audiometry
Phonetically balancedword list( monosyllabic words or bisyllabic words ) words
must be covered in patients language.
Speech Detection Threshold (SDT) = lowest level of speech can be detected at
50% of times (normal = PTA (+/- 10dB )
Speech reception threshold (SRT) = lowest level of speech can be identified
and repeated corrctyl at 50% of times (Normal <25 dB)
Speech discrimination score (SDS ) /WRS = percentage of correctly identified
words.
Normal score is 90 to 100% ,
Conductive 70-80% ,
Sensory L 50-60 %
In neural loss SDS is low. (< 50 % )
ROLLOVER INDEX
??
*
It isseen in retro cochlear hearing loss
*
With increase in speech intensity above a particular level, the word
score fall rather than maintain a plateau as in cochlear type of hearing
loss
28.
*
If the patientis not a native language speaker, you may
need to skip speech audiometry and note why didn't perform
speech testing on the audiogram
*
If you have hearing loss (as the tester) you may have
difficulty hearing what the patient said
*
Don't be afraid to ask the patient for clarification on a word
or to use the word in a sentence if you aren't sure what
they said
*
Have the patient face you so you can read their lips just
make sure they can't see your lips if you aren't using a
recorded list
)
Limitations of speech audiometry
2. Eustachian tubefunction tests
Eustachian tube dysfunction is a
condition where the tubes that
connect middle ears to upper throat
become blocked. This can lead to
discomfort, hearing difficulties and a
feeling of fullness in ear.
33.
3. acoustic stapedialreflex tests
This objective test is to make sure that the stapedius muscle in your middle
ear is functioning correctly and providing a protective mechanism by
stablising the hearing bones of the middle ear by contracting to loud sounds
34.
Otoacoustic Emissions (OAE)
OAE are low-intensity sounds/acoustic signals that
are generated by the cochlea and propogate through
the middle ear into the ear canal where they are
recorded
OAEs are probably not essential to hearing, but
rather are the byproduct of active processing by the
outer-hair cell system.
They are most probably generated by active
mechanical contraction of the outer hair cells,
spontaneously or in reponse to sound.
OAEs reveal, with considerable sensitivity, the
integrity of outer-hair cell function
35.
TYPES OF OAE
Spontaneous otoacoustic emissions (SOAEs) - Sounds emitted without an
acoustic stimulus (ie, spontaneously).
Transient otoacoustic emissions (TOAEs) or transient evoked otoacoustic
emissions (TEOAEs) - Sounds emitted in response to an acoustic stimuli of very
short duration; usually clicks but can be tone-bursts.
Distortion product otoacoustic emissions (DPOEs) - Sounds emitted in response
to 2 simultaneous tones of different frequencies.
Sustained-frequency otoacoustic emissions (SFOAEs) - Sounds emitted in
response to a continuous tone.
Auditory Brainstem Response(ABR
A diagnostic Auditory Brainstem Response (ABR) is a test that
looks at neural responses to sound to determine whether lesions
or other abnormalities exist in the ear, along the auditory nerve,
or in the brainstem. Some wires are taped to the patient's scalp
and ears and connected to a computer
Hearing assessment inchildren
The diagnostic test used depend on the child chronological & developmental age
1-Distraction test. (6-8 M.)
2- (Co-operative) test.
Visual Reinforcement Audiometry (VRA) (8-30 M.)
3-Performance test (play conditioning
Audiometry ). ( > 30 M.)
4- F.F. speech discrimination tests..... under 5Y.
4-PTA. > 5 Y
6-Impedance measure.:
7-OAEs.
8-ABR
40.
06/16/2025 40
Reading sources
1-HCHA 101-4 Hearing Evaluation Procedures 21 pages.
2- AUDIOLOGY the fundamentals cha 4 p 101 -131.
3- Old book (Audiometery) papers.
4- Audiology for practice 2 books for how to interpret PTA.
5- Audiology DIAGNOSIS by Ross J.Roeser cha11,page 227-249.
6- Scott- Brown p 3260 -3274)
7-Kramer. S, and Brown, D. (2019)
8- Audiology Science to Practice (
41.
06/16/2025 41
Reading sources
1-HCHA 101-4 Hearing Evaluation Procedures 21 pages.
2- AUDIOLOGY the fundamentals cha 4 p 101 -131.
3- Old book (Audiometery) papers.
4- Audiology for practice 2 books for how to interpret PTA.
5- Audiology DIAGNOSIS by Ross J.Roeser cha11,page 227-249.
6- Scott- Brown p 3260 -3274)
7-Kramer. S, and Brown, D. (2019)
8- Audiology Science to Practice