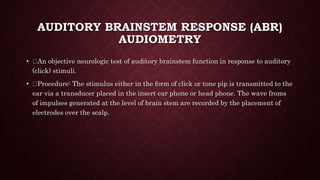
This document provides an overview of approaches to deafness, including types and causes of hearing loss, diagnosing hearing loss through various tests, and managing different types of hearing loss. It discusses conductive hearing loss due to defects in the outer or middle ear, sensorineural hearing loss due to inner ear or nerve problems, and mixed hearing loss. Common causes include presbycusis, noise exposure, meningitis, and ototoxic drugs. Diagnostic tests include tuning fork tests, pure tone audiometry, impedance testing, and brainstem response audiometry. Management involves hearing aids, cochlear implants, assistive devices, and training programs.


















![• PURE TONE AUDIOMETRY (PTA
• PTA is the key hearing test used to identify hearing threshold level of an
individual, enabling determination of the degree, types and configuration of hearing
loss.
• Provides the basis for diagnosis and management. The symbols used on most
audiograms are: x - left, air conduction o - right, air conduction ] - left, bone
conduction [ - right, bone conduction](https://image.slidesharecdn.com/approachtodeafness-201105093312/85/Approach-to-deafness-21-320.jpg)