Downloaded 137 times

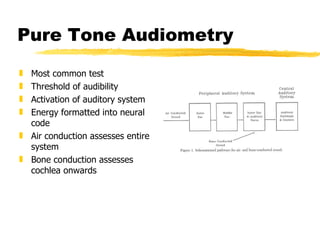

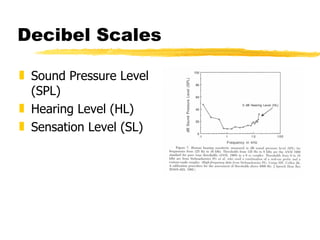




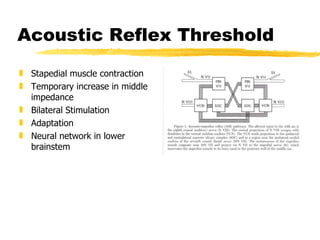









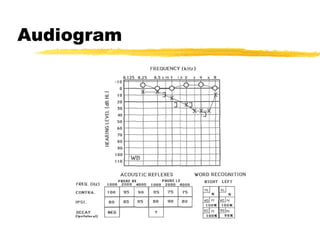


This document summarizes various auditory tests used to assess peripheral and central auditory function. It discusses pure tone audiometry, tympanometry, acoustic reflex measurements, electrocochleography, auditory brainstem response testing, and otoacoustic emissions. As an example, it presents the case of a 31-year-old male found to have a left-sided acoustic neuroma based on audiogram findings, elevated ipsilateral and contralateral reflexes on the left side, and MRI results.























































































