Downloaded 1,181 times
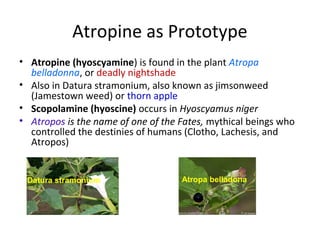
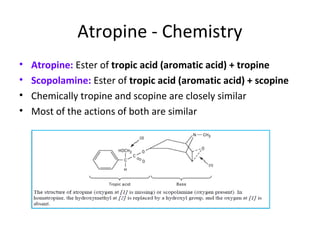

The document discusses anticholinergic drugs, focusing on their classification, mechanisms of action, pharmacokinetics, and therapeutic uses. It highlights atropine and its synthetic derivatives' effects on various systems, including the CNS, cardiovascular system, and smooth muscles, while also addressing potential adverse effects and contraindications. Additionally, it covers ganglion-blocking drugs and nicotine's role in smoking cessation pharmacotherapy.



























































































![CASE_PRESENTATION_ON_subdural_hematoma(SDH)[1 FINAL PPT]-1.pptx](https://cdn.slidesharecdn.com/ss_thumbnails/casepresentationonsubduralhematomasdh1finalppt-1-260129172522-d405d375-thumbnail.jpg?width=640&height=640&fit=bounds)















