Downloaded 103 times
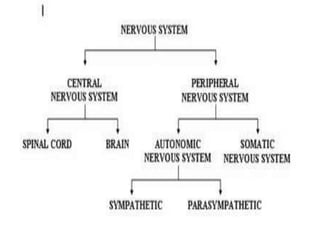
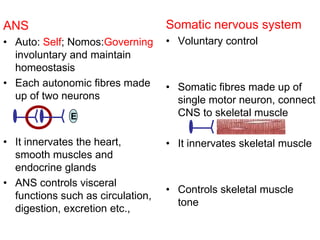
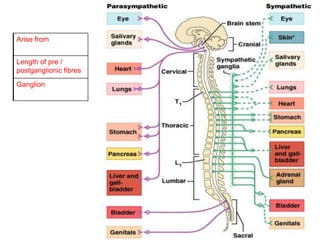
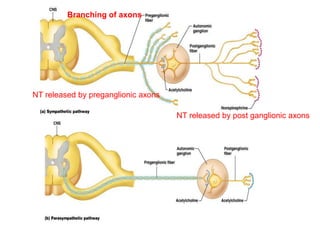
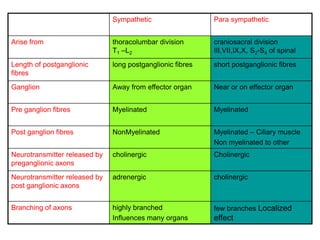
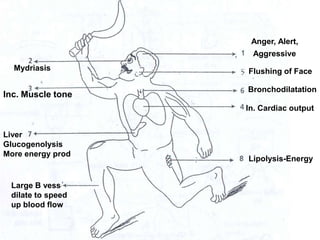
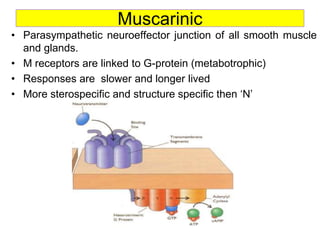
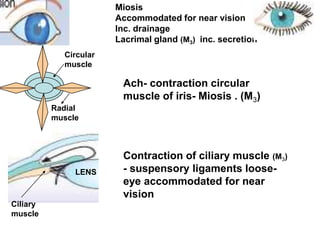
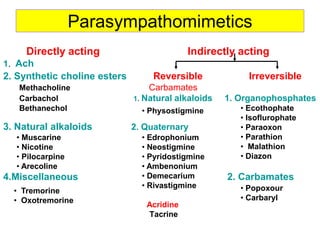
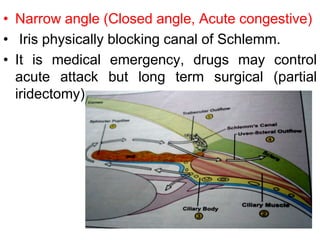
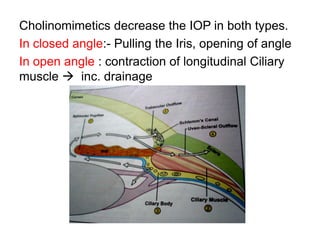
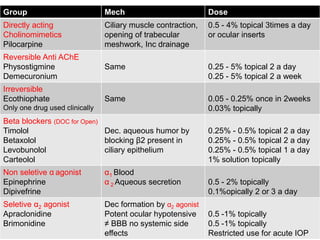
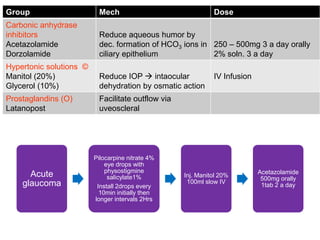
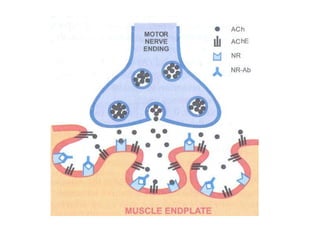


The document discusses the nervous system, specifically focusing on the peripheral nervous system (PNS) and its divisions - the autonomic nervous system (ANS) and somatic nervous system. It provides details on the ANS, including its sympathetic and parasympathetic divisions. The parasympathetic system uses acetylcholine as its neurotransmitter which acts on nicotinic and muscarinic receptors. Cholinergic drugs that act as parasympathomimetics are used to treat various conditions like glaucoma. Pilocarpine is commonly used as a parasympathomimetic eye drop to reduce intraocular pressure in glaucoma by contracting the ciliary muscle and increasing drainage of aqueous humor through the trabecular


















































































![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)











