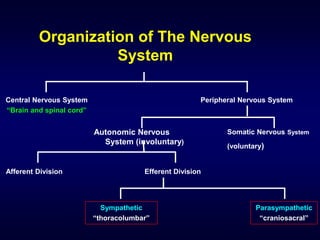
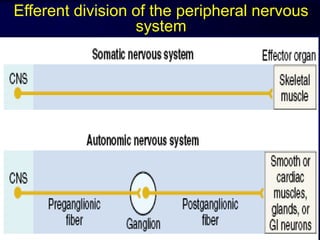
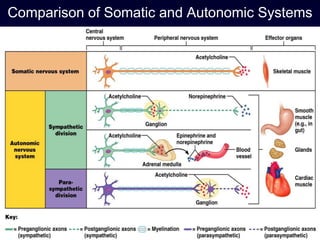
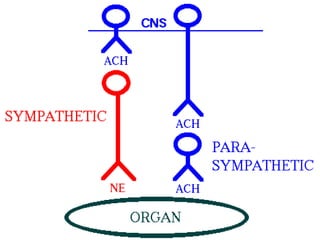
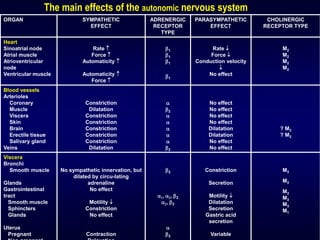
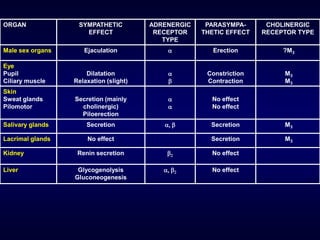
The autonomic nervous system has two main divisions - the sympathetic and parasympathetic nervous systems. The sympathetic nervous system is responsible for the "fight or flight" response and activates processes like increased heart rate and dilation of bronchioles. The parasympathetic nervous system is responsible for "rest and digest" functions like decreased heart rate and activation of gastrointestinal and genitourinary functions. Both systems use neurohumoral transmission using acetylcholine and norepinephrine as neurotransmitters which act on nicotinic and muscarinic receptors. There are many drugs that can selectively target components of the autonomic nervous system including parasympathomimetics, parasympatholytics, sympathomimetics, and sympathol