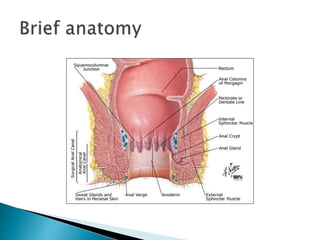
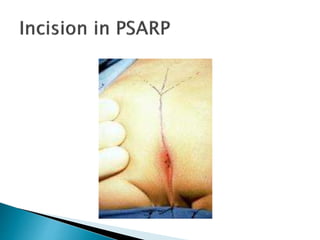
This document provides an overview of anorectal malformations. It begins with an anatomical description of anal canal development. It then discusses the epidemiology and etiology of anorectal malformations. The document classifies anorectal malformations and describes associated comorbidities. It outlines approaches for clinical evaluation, diagnosis and surgical management. Surgical correction depends on whether the malformation is high or low. The newest surgical technique described is posterior sagittal anorectoplasty.