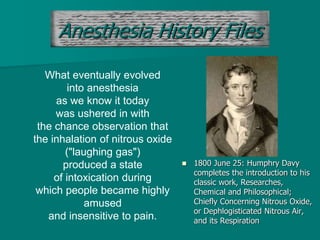
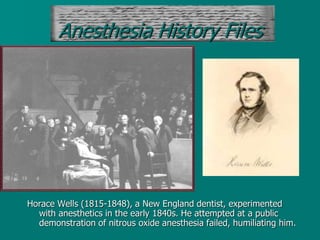
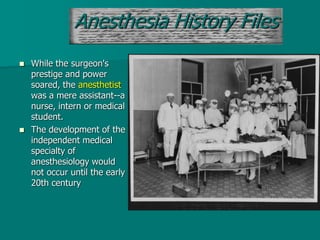
The document discusses the history of anesthesia from ancient times when pain was seen as punishment to modern times when anesthesia allowed for safer surgeries. It describes key events like the first use of ether and other substances for anesthesia. The role of anesthesiologists is also summarized, from providing pain management and life support during surgery to treating acute and chronic pain.