This document provides information on spinal anesthesia, including:
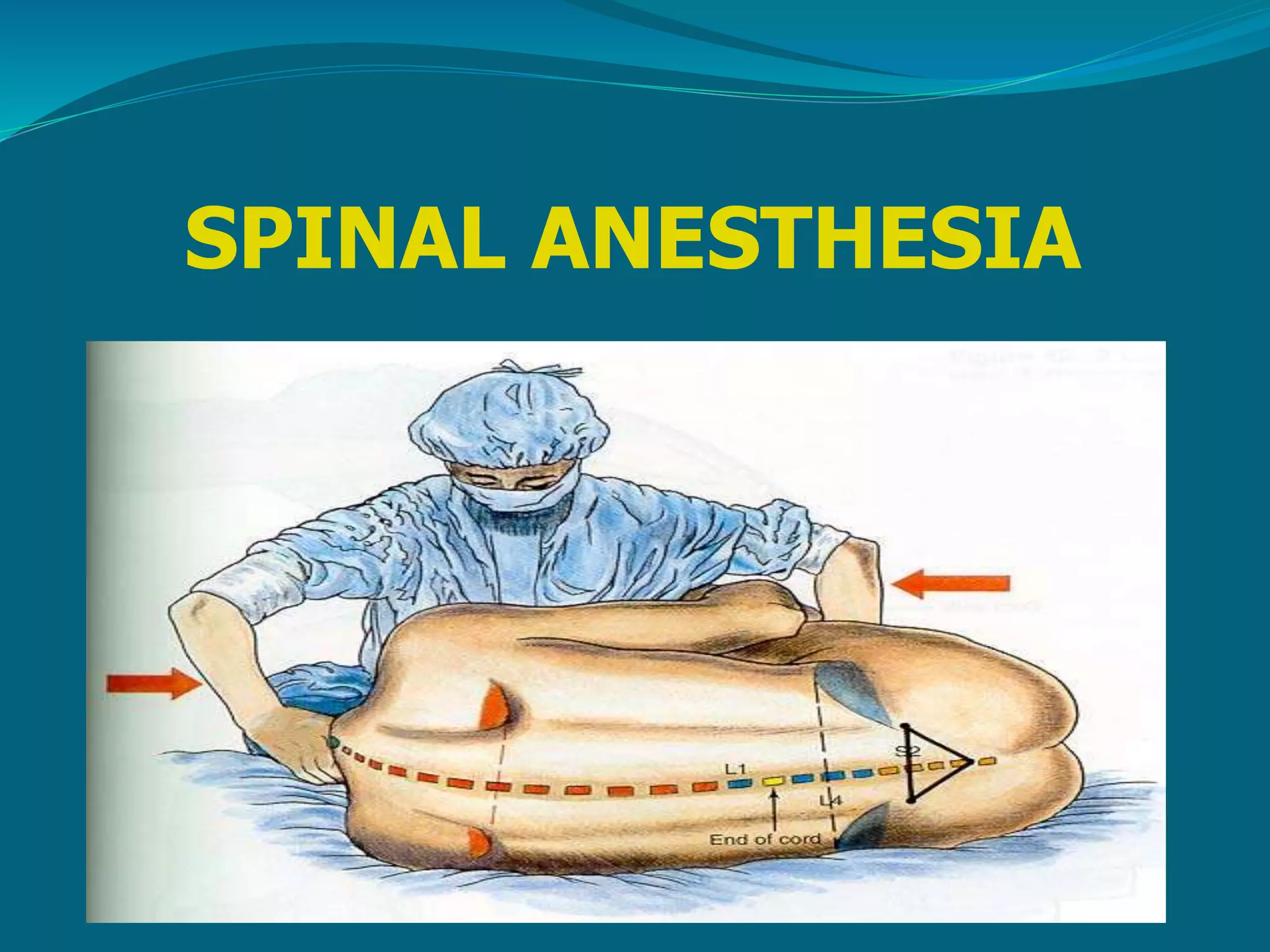
- It involves injecting local anesthetic into the subarachnoid space to block spinal nerve roots and produce sympathetic block, sensory analgesia, and motor block.
- It is used for surgery on the lower half of the body, abdomen, perineum, lower extremities, and vaginal/C-section deliveries. Contraindications include bleeding disorders and increased intracranial pressure.
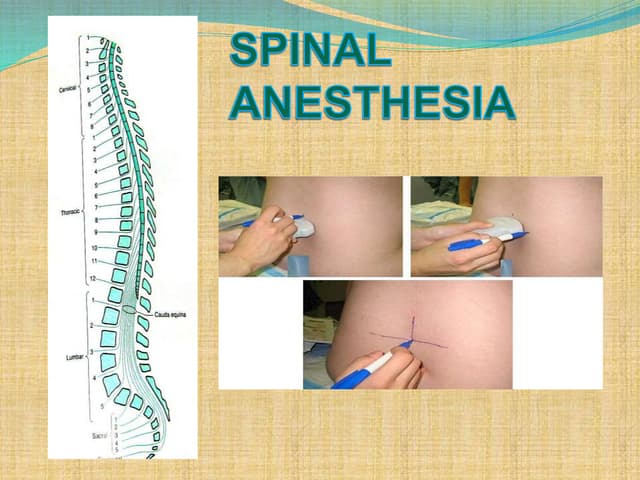
- Common drugs used are tetracaine, lidocaine, and bupivacaine. The level of anesthesia is determined by factors like volume, concentration, speed of injection, and patient position. Potential complications include hypotension, nausea