ANORECTAL MALFORMATION:
Absence ofanus in the perinium is traditionally
known as imperforated anus.Now this
anomaly termed as anorectal
malformation(ARM).
3.
HISTORY AND INCIDENCE:
In 1980 Alberto Pena for the first time
performed a posterior sagittal approach for the
treatment of a baby with imperforated anus.
Average incidence worldwide is 1 in 5000 live
births.
Slightly more common in males.
Embryology:
The cloaca isfirst formed at around 21 days
gestation.It is U shaped, with the allantois
lying anteriorly and the hindgut posteriorly.
At 6th
weeks a urogenital cavity anteriorly and
an anorectal cavity posteriorly formed.
At 7th
weeks cloacal membrane breaks down
and creating two opening the urogenital and
anal opening.
6.
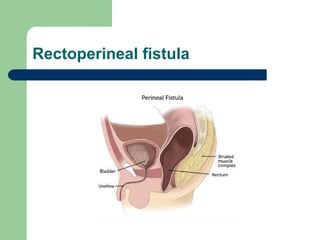
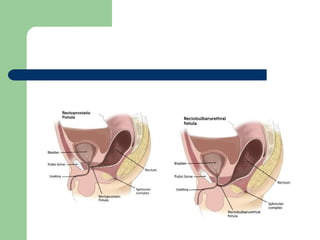
RECTOPERINEAL FISTULA….
It isthe lowest type of defect.Rectum is located within
most of the sphincter mechanism.
Sometimes fistula does not open into the perineum but
rather follows a subepithelial midline tract,along the
midline raphy,scrotum or even at the base of the
penis.
The termed covered anus,anal membrane,anteriorly
mislocated anus, and bucket handle malformations all
refer to rectoperineal fistula.
Rectourethral fistula:
ARM withrectourethral fistula is the most common defect in
males.The fistula may be located at the lower bulbar or
the higher prostatic part of urethra.Lower urethral fistulas
are usually associated with good quality muscles,a well
developed sacrum,a prominent midline groove,and a
prominent anal dimple.High urethral fistula associated
with poor quality muscles,abnormally developed sacrum,a
flat perineum,poor midline groove,and a barely visible
anal dimple.
10.
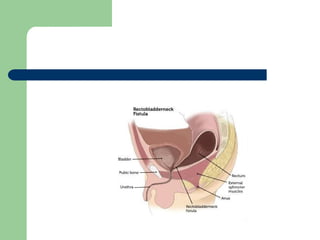
Rectobladder neck fistula:
Inthis defect ,rectum opens into the bladder neck.Usually caries a
poor prognosis for bowel control because musles and external
sphincter are poorly developed.Sacrum is often deformed and
short,perineum is often flat.About 10% males fall into this
category.
12.
Anorectal atresia withoutfistula:
Most patients with this defect have a good
prognosis for bowel function.Rectum usually
ends blindly 2 cm from the perineal skin.Rectum
and urethra seperated by a thin common
wall.About half of the patients with no fistula
have Down syndrome.
13.
Rectal atresia/Rectal stenosis:
Thisis unusual defect in males <1%.The lumen
of rectum is totally or partially interrupted,The
upper pouch is a dilated rectum and the lower
portion empties into a small anal canal that is
the normal location.These two rectal
structures may be separated by a thin
membrane or by dense fibrous tissue.Patients
with these defect have an excellent functional
prognosis>
14.
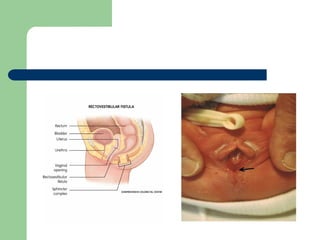
Rectovestibular fistula:
Rectovestibular fistulais the most common defect in females and an
excellent functional prognosis.A meticulous inspection allows the
clinician to see that there is a normal urethral meatus and a
normal vagina,with a third hole in the vestibule.About 5% of these
patients will have two hemivaginas with a vaginal septum.This
defect can be repaired without a protective colostomy.
16.
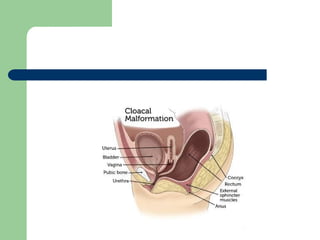
Cloacal malformation:
A cloacais the extreme in the spectrum of
complexity of female malformations and
occurs when the distal portion of the
rectum ,vagina and urinary tract fuse and
create a common channel.The length of
common channel varies from 1-8 cm.A
common channel of <3 cm means this defect
can repair with a posterior sagittal approach.
18.
Continue:
Common channel>3 cm are more complex
and need abdominal approach to mobilize
structures.Short common channel have good
prognosis and long common channel habe
bad prognosis.
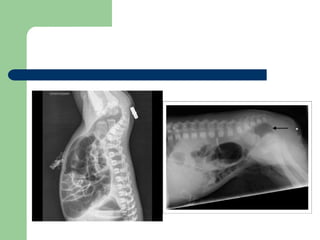
Investigation:
Invertogram
Cross-tablelateral x-ray
Following are evaluated on Invertogram:
Level of gas in the blind rectal pouch :
If above P-C Line:Indicates low anomaly
If below P-C Line:Indicates High anomaly
Sacral anomaly
Bowel loop pattern
Postoperative care:
Inthe absence of laparatomy,oral feeding may begin
when the child awake.
Antibiotics are given for 48 hours
In males who had a rectourethral fistula,the urinary
catheter should be left in place for 7 days.
Incase of cloacal repair the urethral catheter left in
place for 2 to 3 weeks
Dilatation program is begun 2 weeks after surgery
Initially dilator is used twice a day,every week,the size
of the dilator is increased by one unit until the desired
size is reached.
26.
CONTINUE…
Once thecorrect size is reached,the colostomy can
be closed,which is usually 8 to 12 weeks after
reconstruction.
Dilatation must be continue after closure.once the
dilator can be inserted easily,the schedule is reduced
to once a day for 1 month,twice a week for 1
month,once a week for 1 month,and then once a
week for 3 month.
27.
Anal dilatation program:
Patient age
1-4 month
4-8 month
8-12 month
1-3 yr
3-12 yr
>12 yr
Hegar dilator
Size 12
Size 13
Size 14
Size 15
Size 16
Size 17
28.
Complications:
Wound infection
Wound dehiscence
Anal stricture may be the cosequenceof leaving the
anoplasty under tension or inadequate blood supply.
Constipation
Rectal prolapse
Urethrovaginal fistula incase of cloacal repair
Neurogenic bladder due to dissection of the rectum in the
wrong plane