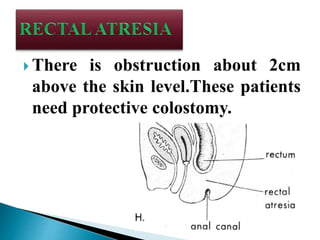
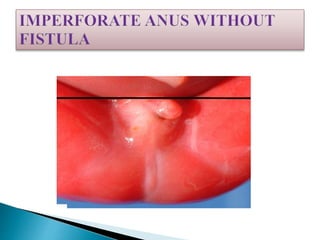
Anorectal malformations are congenital defects that occur during gestation when the rectum fails to descend and connect to the anal opening. They range from mild defects like anal stenosis to more severe ones like rectal atresia. Treatment involves surgical correction like colostomy followed by anoplasty. Nursing care focuses on wound, stoma and postoperative bowel care to support healing and prevent complications.