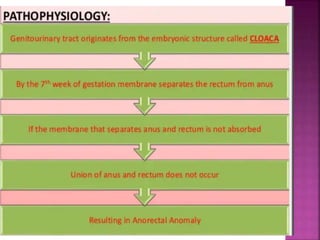
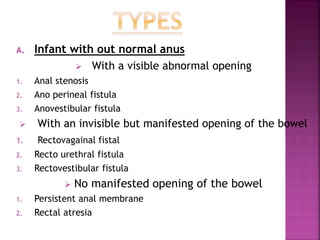
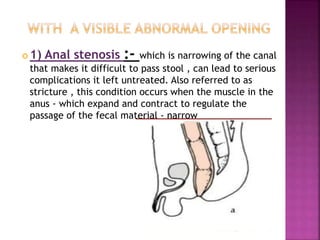
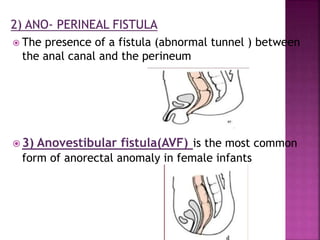
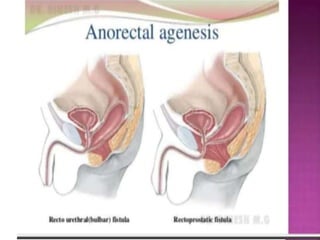
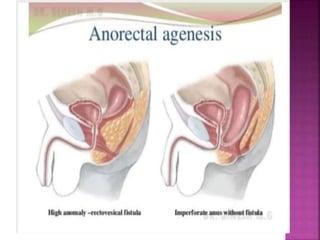
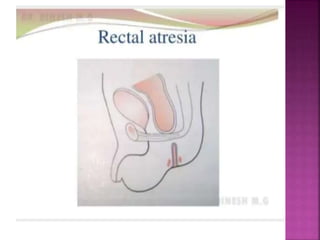
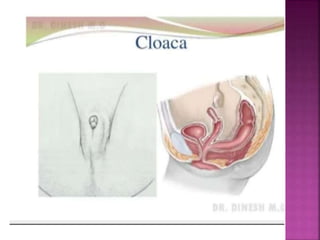
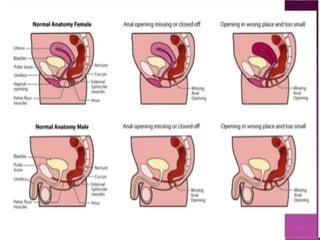
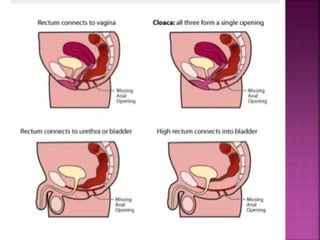
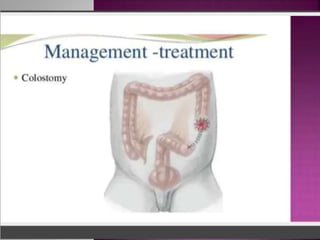
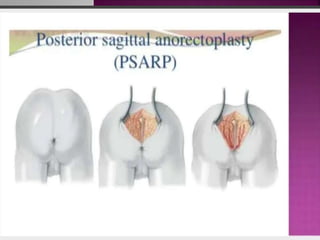
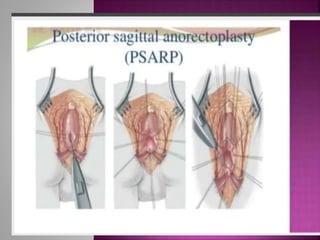
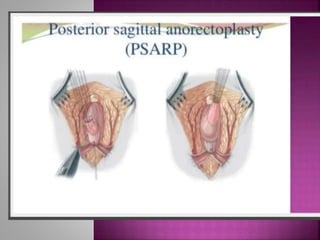
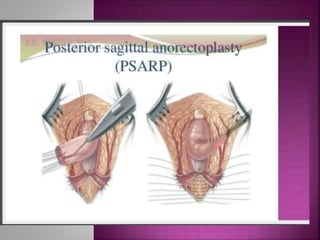
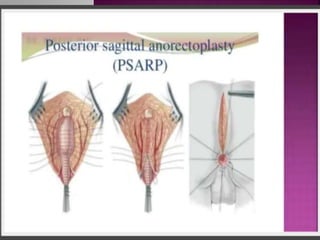
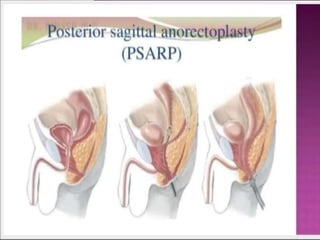
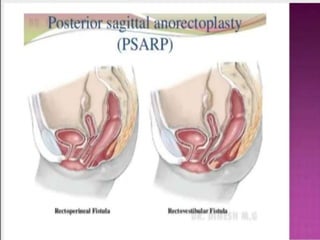
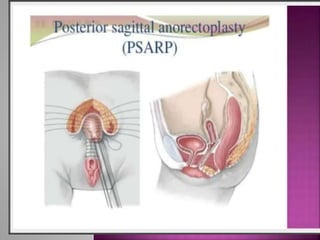
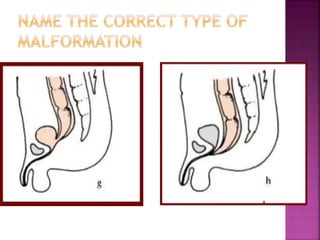
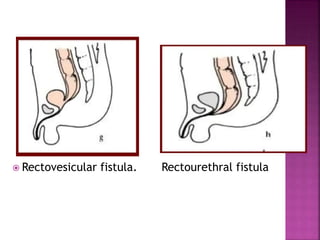
The document discusses anorectal malformations in children. It defines anorectal malformations as anomalies of the rectum and distal anus that can range from simple imperforate anus to complex anomalies involving the genitourinary and pelvic organs. Signs may include failure to pass meconium or stool leaking through abnormal openings. Treatment involves stabilization, surgery such as colostomy or posterior sagittal anorectoplasty, and lifelong bowel management. Postoperative care focuses on meticulous perineal care and prevention of complications.