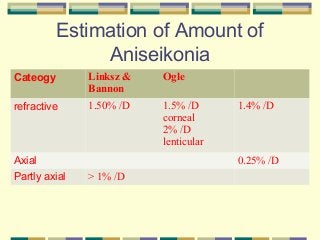
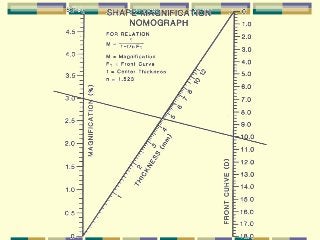
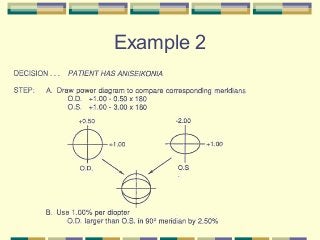
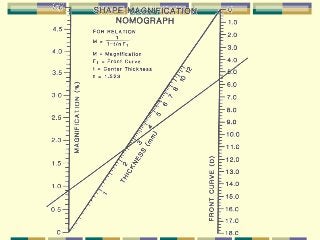
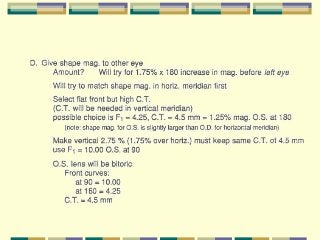
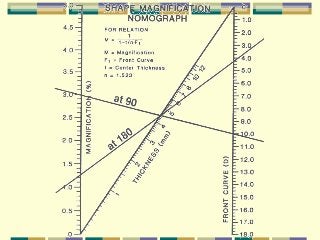
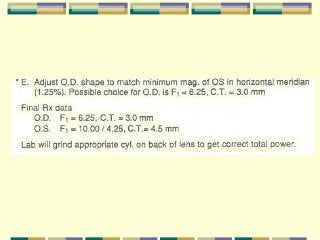
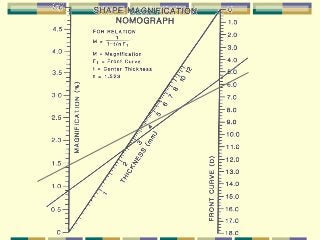
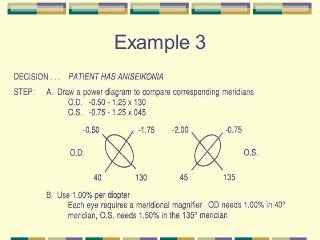
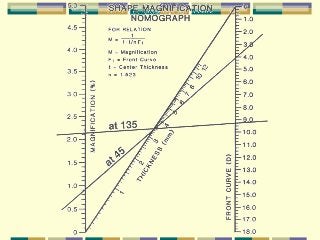
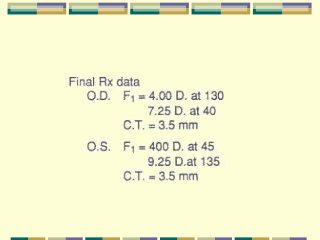
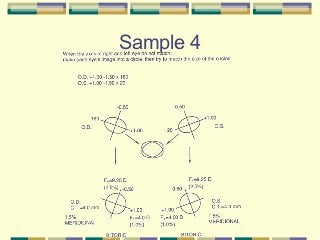

This document discusses aniseikonia, which is a difference in the size or shape of retinal images between the two eyes. It can be caused by refractive errors, corneal issues, lenticular problems, or axial length differences. Aniseikonia affects 2-3% of the population and can induce symptoms like headaches, eyestrain, and difficulties with depth perception. The document provides guidelines for evaluating and managing aniseikonia, including formulas for calculating spectacle and contact lens magnification to help reduce the perceived size difference between eyes. It also includes examples of calculating lens parameters to minimize aniseikonia for different refractive error scenarios.













































![Aniseikonia [ophthalmology description for medical students ]](https://cdn.slidesharecdn.com/ss_thumbnails/aniseikonia-201008163906-thumbnail.jpg?width=640&height=640&fit=bounds)









































