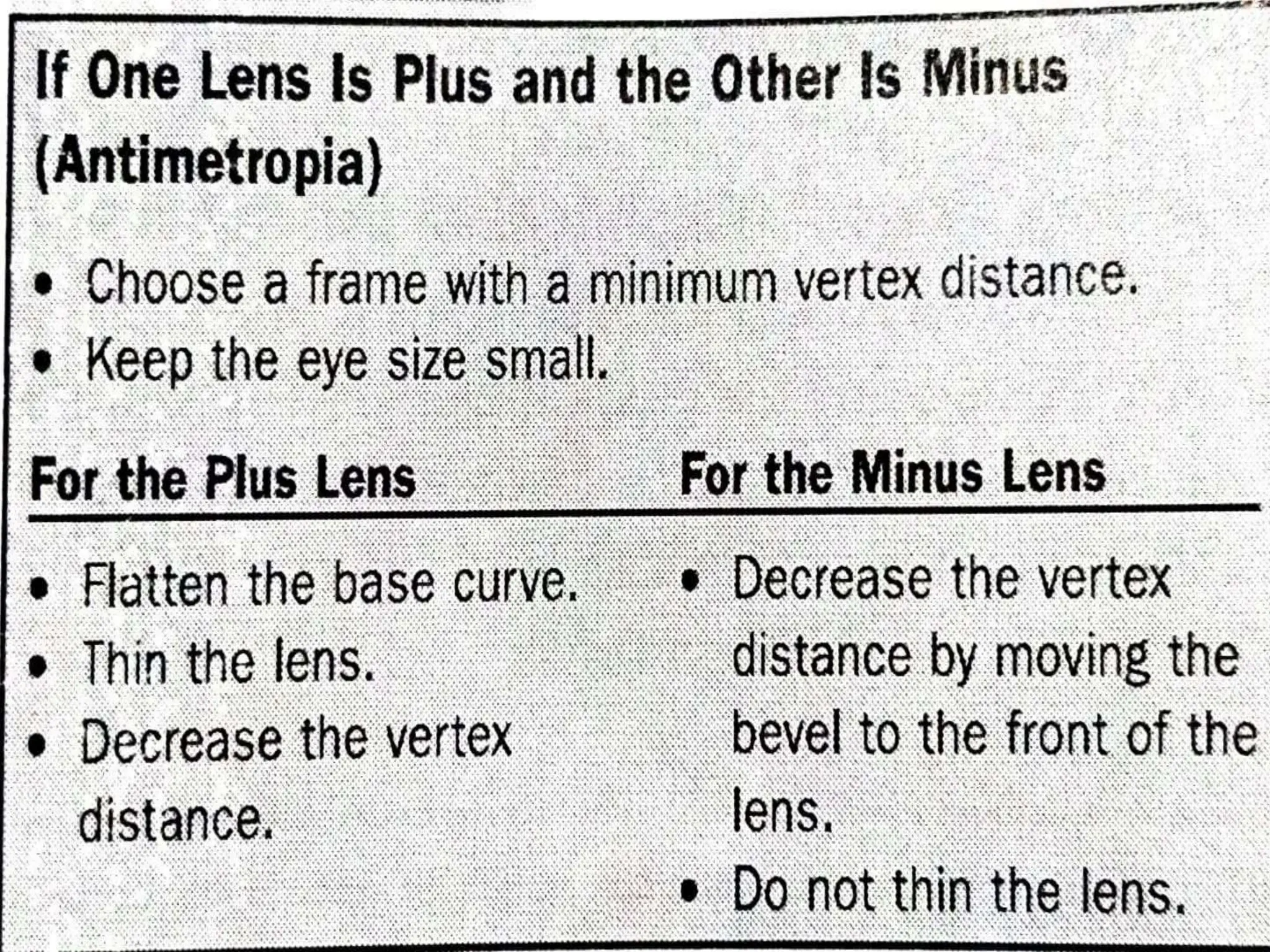
The document discusses anisometropia, a condition characterized by differing refractive power between the eyes, and its effects on vision, especially in relation to presbyopia. It explains aniseikonia, which is the perceived difference in image size between the two eyes, and highlights the importance of detecting and prescribing corrective measures for patients who experience this condition. Additionally, it provides guidelines for lens design and the methods to correct aniseikonia, emphasizing the significance of customizing lenses to improve visual comfort.






























































![Aniseikonia [ophthalmology description for medical students ]](https://cdn.slidesharecdn.com/ss_thumbnails/aniseikonia-201008163906-thumbnail.jpg?width=640&height=640&fit=bounds)
































