Downloaded 873 times














![Rupture outcomes
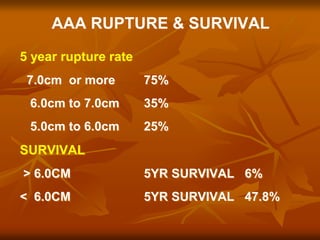
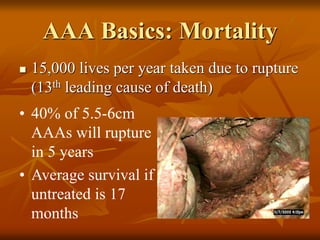
Mortality rate can be as high as 80%[1]
More than one third of rupture cases die outside the
hospital
Ruptured AAA
1. Adam. J Vasc Surg 1999;30:922-8.
2. Thomas. Br J Surg Aug 1988](https://image.slidesharecdn.com/joy-160510125440/85/Aneurysm-109-320.jpg)




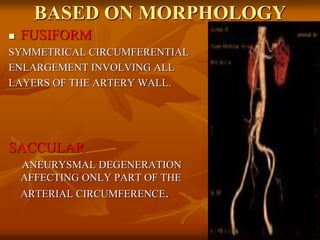
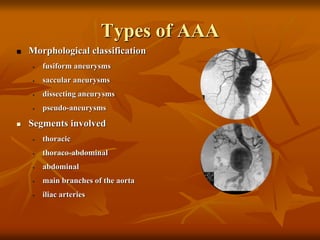
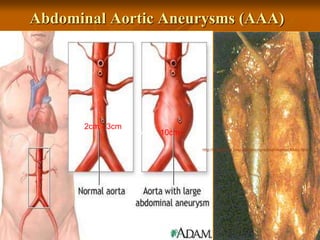
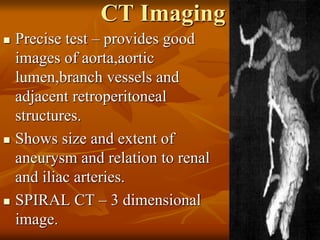
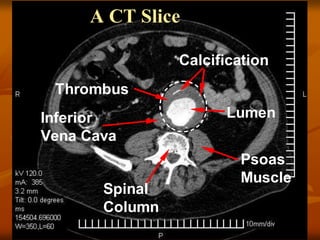
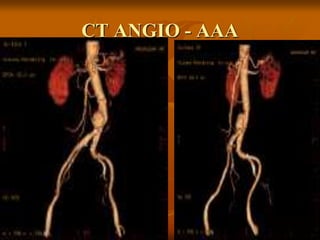
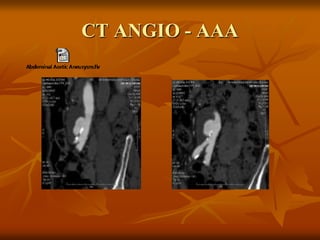
The document outlines a seminar presentation on aneurysms. It discusses the introduction, historical aspects, classification, abdominal aortic aneurysm, surgical management, and recent advances related to aneurysms. The presentation covers the definition, etiology, location, morphology, and pathogenesis of different types of aneurysms. It provides details on abdominal aortic aneurysms including risk factors, natural progression, clinical presentation, diagnosis using imaging modalities like ultrasound and CT, and treatment.
































































































