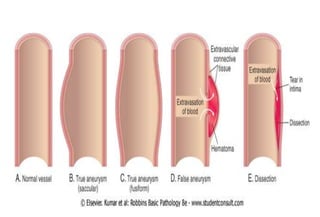
An aortic aneurysm is a localized sac or dilation formed at a weak point in the aortic wall. They most commonly occur in the abdominal aorta and can be caused by conditions like hypertension, atherosclerosis, and smoking. Aortic aneurysms are classified as either saccular or fusiform based on their shape and size. Untreated aneurysms risk rupture, which can cause massive hemorrhage and death. Surgical treatment involves replacing the diseased aortic segment with a synthetic graft to prevent rupture.



















































































![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)






