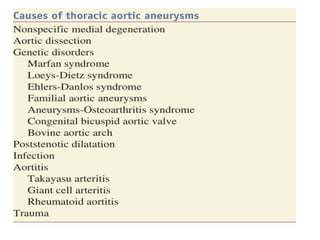
A retired colonel presented to the emergency room with chronic chest pain. Further evaluation revealed he had a massive haemothorax secondary to a ruptured aortic aneurysm. Autopsy showed aortic aneurysms are caused by alterations to the delicate balance in the aortic wall that leads to dilatation. Thoracic aortic aneurysms are generally repaired electively when they reach a diameter of 6 cm or greater to prevent fatal rupture. Treatment options include open surgical repair or endovascular stent graft placement depending on the location and extent of the aneurysm.