Downloaded 228 times




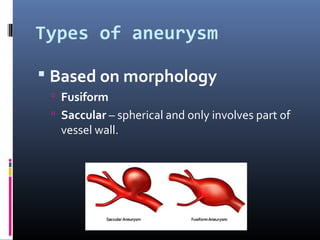































The document discusses arterial aneurysms, defining them as abnormal dilations of blood vessels and classifying them based on morphological and locational characteristics. It highlights abdominal aortic aneurysms (AAA) as common in older males, often caused by atherosclerosis, and outlines diagnosis and management strategies, including imaging techniques and surgical options. Complications from aneurysms and their repair, such as bleeding and cardiac events, are also detailed.