Downloaded 31 times

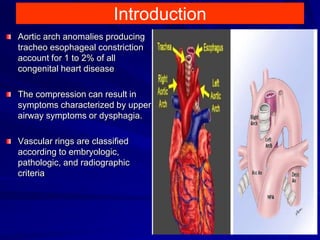
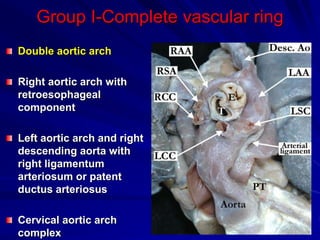
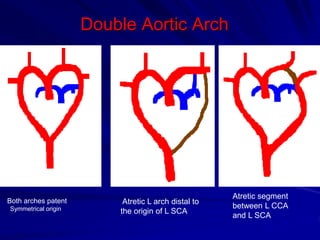
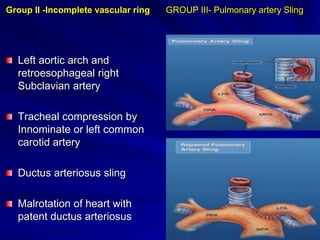
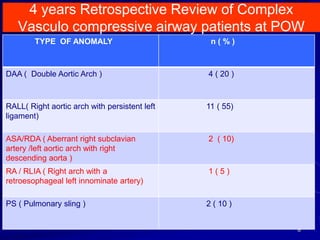
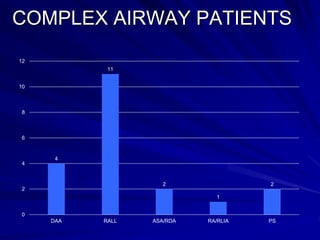
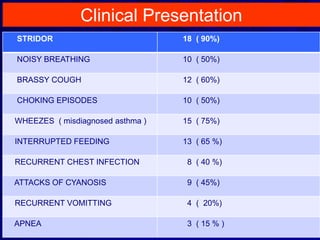


This document discusses vascular compressions of the airways, specifically double aortic arches and right aortic arch anomalies. It presents 4 case studies of pediatric patients presenting with airway symptoms due to these conditions. The first section provides an overview of vascular ring classifications and anomalies that can cause tracheal compression. It also reviews clinical presentations and diagnostic findings. Surgical approaches like division of arches, aortopexy and tracheopexy are described. The importance of a multidisciplinary team in managing these complex airway cases is emphasized.























































































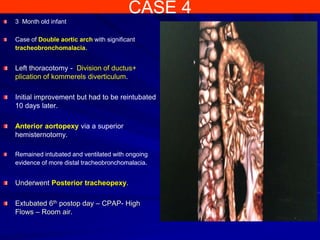
![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)