This document discusses abdominal aortic aneurysms. Key points include:
- Abdominal aortic aneurysms are defined as a dilation of the aorta to over 1.5 times its normal diameter. Risk factors include age over 50 for men and 70 for women, family history, and smoking.
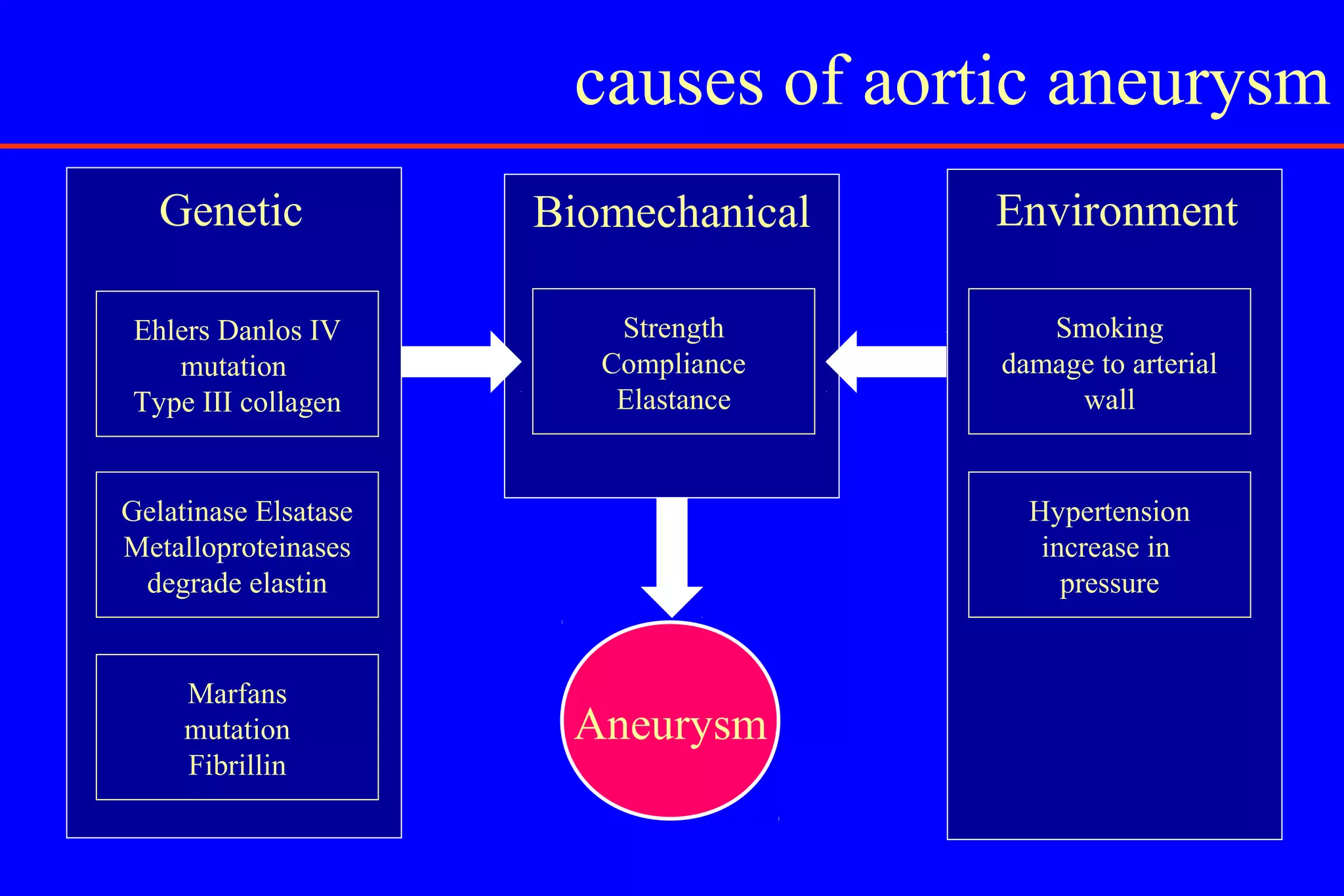
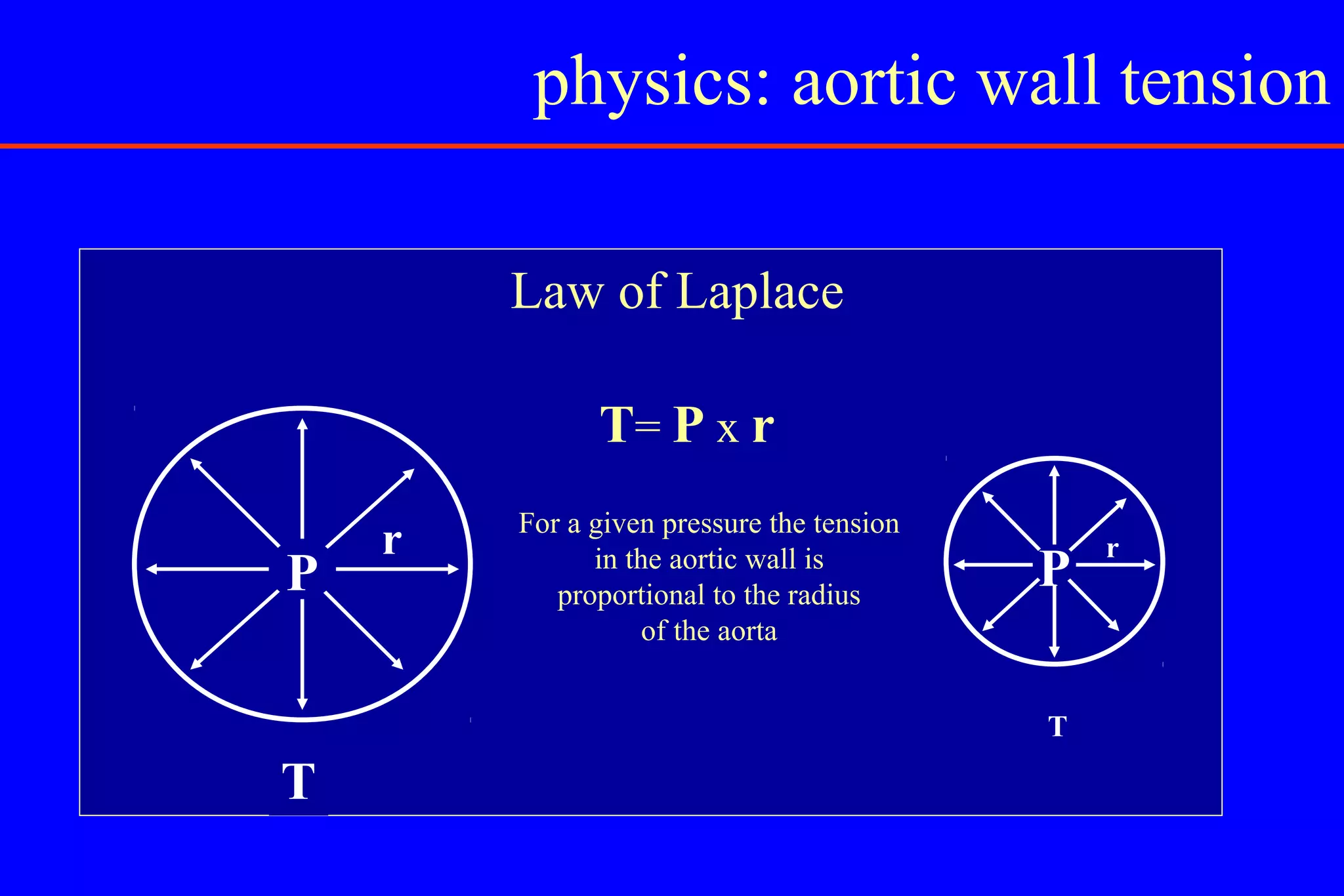
- Aneurysms rupture when the wall tension exceeds the strength of the aneurysm wall, which depends on size, shape, blood pressure, and the material properties of the wall.
- Treatment options include open surgical repair or endovascular stent graft placement. Complications can include cardiac, pulmonary, and renal issues. Late complications include anastomotic failures or new aneurysm formation. Five-year survival after


![aortic aneurysms 2
• Family history
• 15-20% of patients with AAA have a first degree relative
with AAA: compared to 2% of controls
• Incidence
• increasing death rate from rupture over last 30yrs
(increasingly elderly popln, [65+yrs to double by 2025])
• 5% men over 65yrs have AAA (screening)](https://image.slidesharecdn.com/aneurysmnurse-180209123602/75/Abdominal-Aortic-Aneurysm-3-2048.jpg)