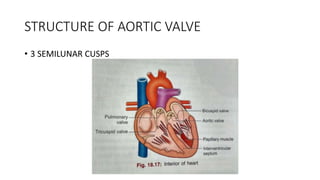
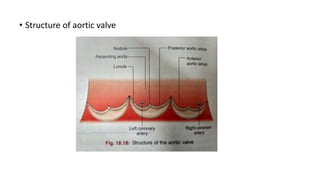
The aortic valve has three cusps that open and close to regulate blood flow from the heart to the aorta. Aortic stenosis occurs when the valve opening narrows due to calcium buildup on the cusps. In the elderly, aortic stenosis is usually caused by age-related degeneration and calcification of the valve. Symptoms include chest pain, shortness of breath, and fainting. Diagnosis involves echocardiogram, Doppler ultrasound and cardiac catheterization. Treatment options include medications, balloon valvuloplasty, open-heart surgery to replace the valve, and newer transcatheter aortic valve replacement procedures for high-risk elderly patients.