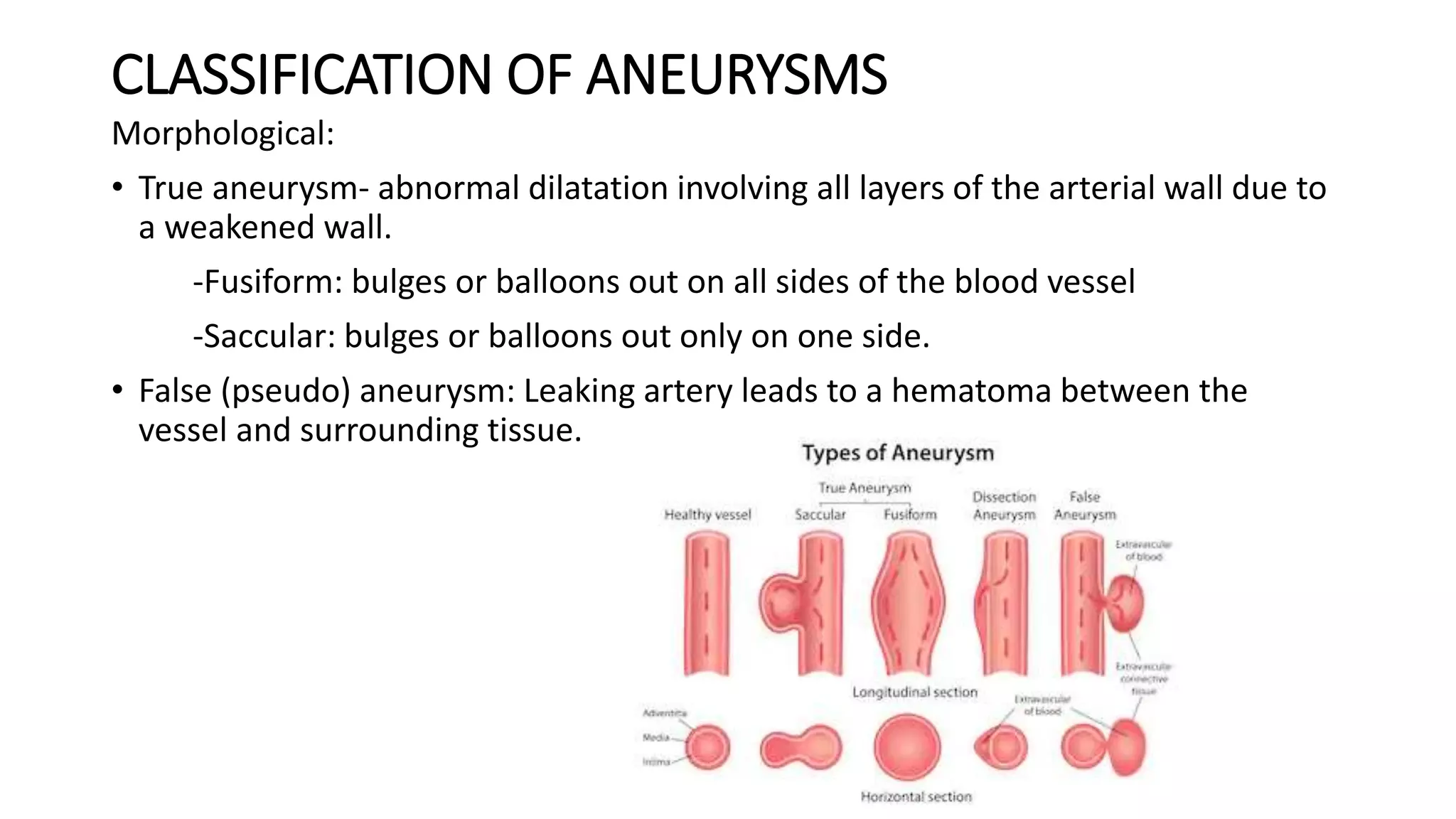
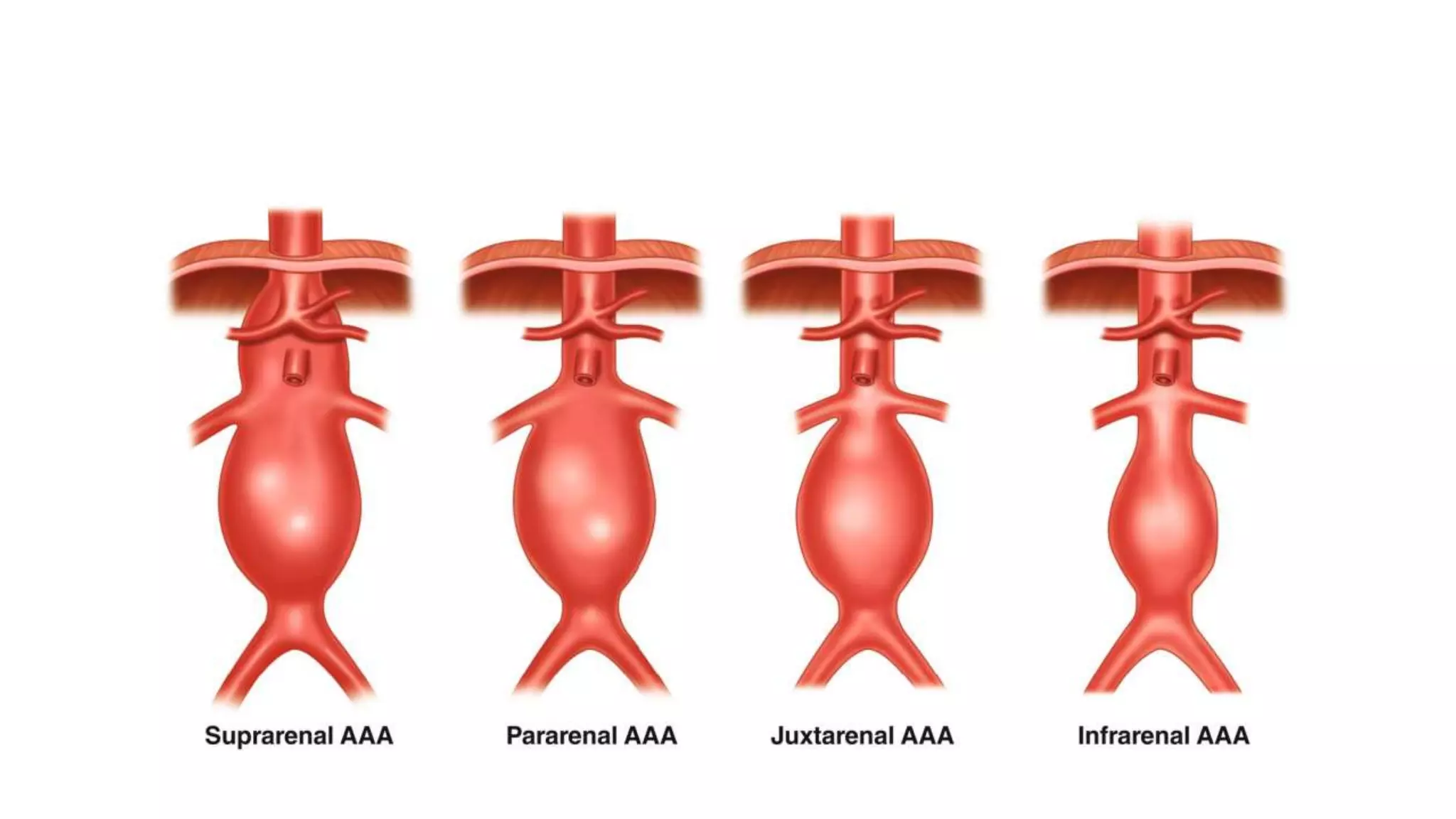
This document provides an overview of abdominal aortic aneurysms (AAA). It defines AAAs as a dilatation of the aorta over 50% of normal diameter. AAAs are classified based on location and morphology. Risk factors include older age, male sex, smoking, and family history. Small AAAs under 4cm are monitored. Larger or symptomatic AAAs require surgical repair, either open surgery or the less invasive endovascular aneurysm repair. The goal of treatment is to prevent AAA rupture, which has a high mortality rate.