Downloaded 1,696 times
![• Before ERCP, all of the patient’s previous abdominal imaging findings
(from CT scans, magnetic resonance imaging [MRI], ultrasonography,
and cholangiography or pancreatography) should be reviewed.
• Deep sedation is desirable during ERCP because a stable endoscopic
position in the duodenum is important for proper cannulation,
therapeutic intervention, and avoidance of complications.](https://image.slidesharecdn.com/ercp-141212185234-conversion-gate01/75/Ercp-7-2048.jpg)
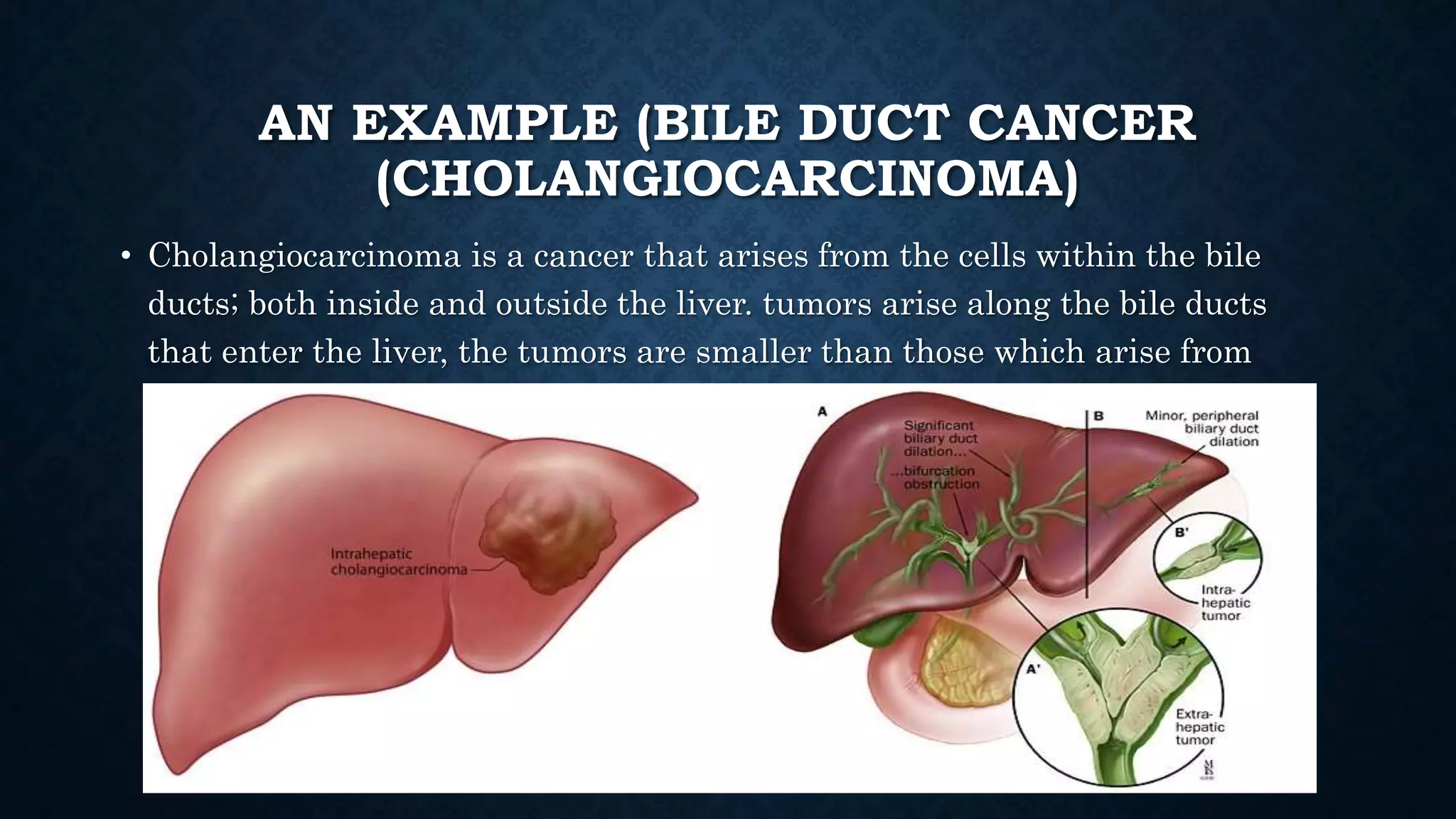
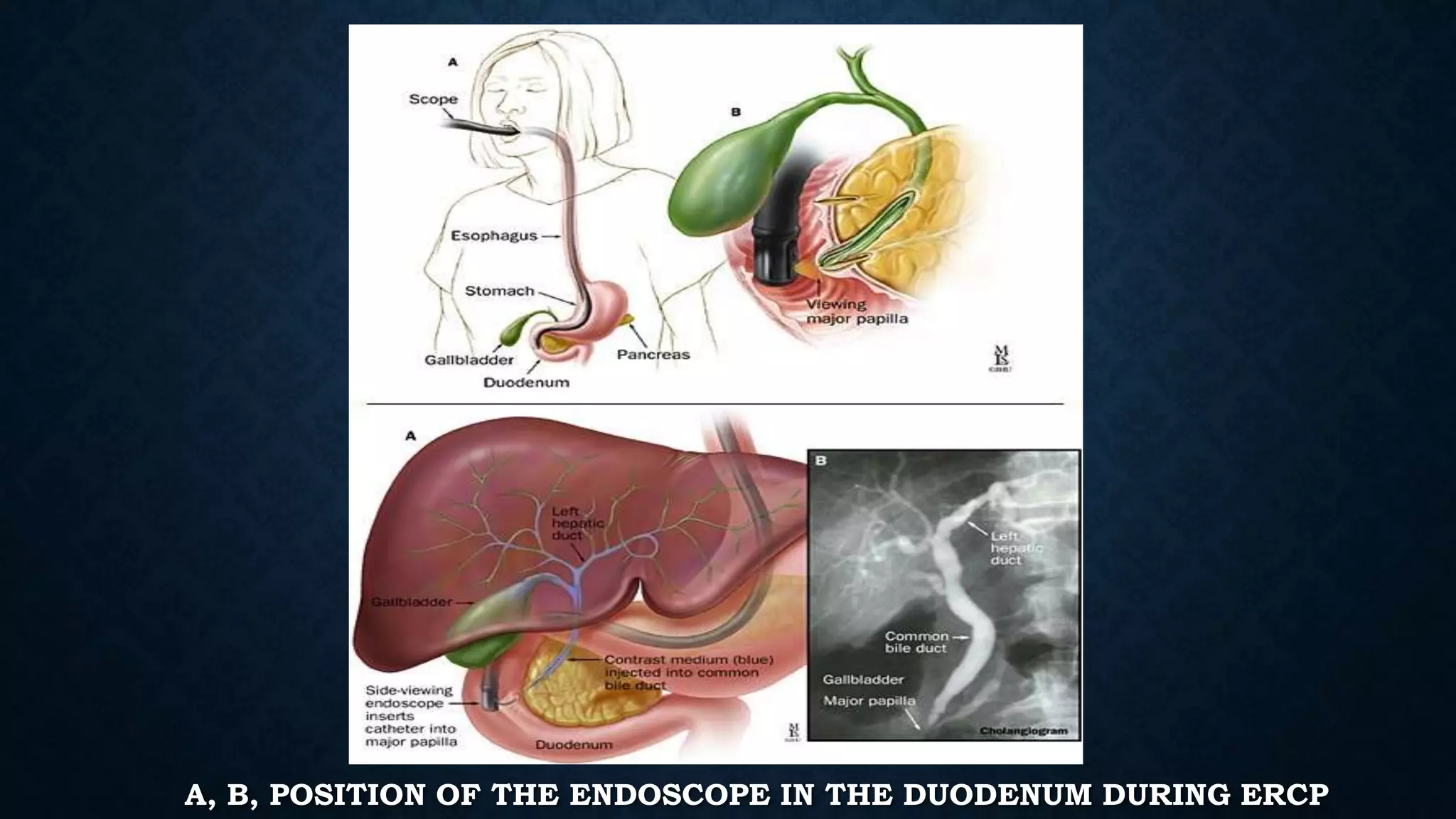


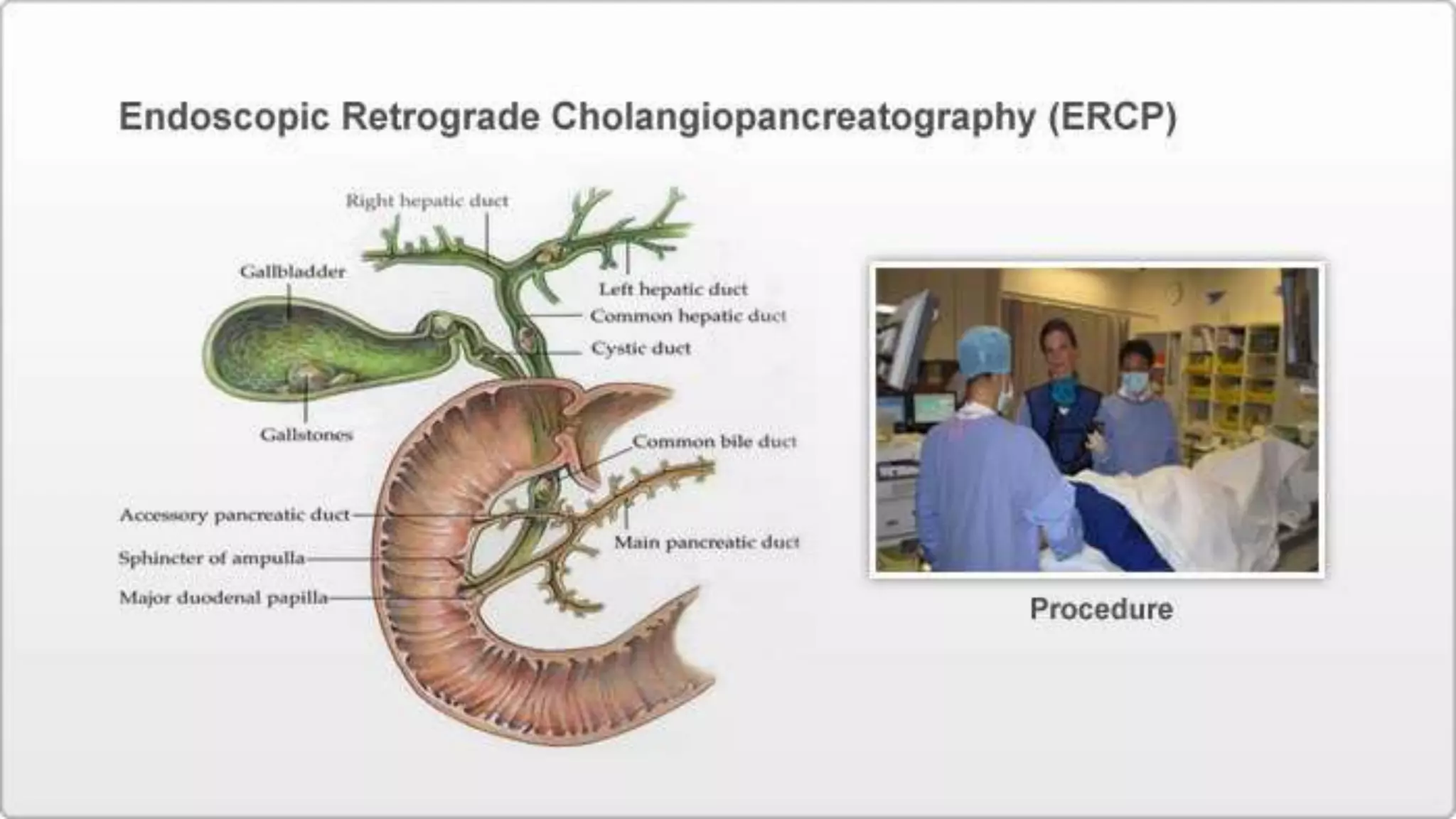
ERCP is an endoscopic procedure that combines endoscopy and fluoroscopy to diagnose and treat issues in the duodenum, bile ducts, pancreatic duct, and gallbladder. During ERCP, an endoscope is inserted and a catheter is used to inject radiocontrast dye to identify any blockages. If needed, a wire can enlarge the opening to the bile duct to remove gallstones or perform other procedures like stent placement. Potential but rare complications include infection, pancreatitis, bleeding, and perforation of the GI tract. ERCP requires an experienced physician due to its risks.













































![define products of ercp-180612090109[1].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/ercp-1806120901091-250602131957-578ccac8-thumbnail.jpg?width=640&height=640&fit=bounds)
![ercp-180612ewdhehwjbfew090109[1][1].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/ercp-18061209010911-250602134756-35275575-thumbnail.jpg?width=640&height=640&fit=bounds)
![definitio products ercp-180612090109[1][1].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/ercp-18061209010911-250602134305-959596a5-thumbnail.jpg?width=640&height=640&fit=bounds)














































