This document describes the components and functioning of an anesthesia machine. It discusses:
- The history of anesthesia machines and their development over time.
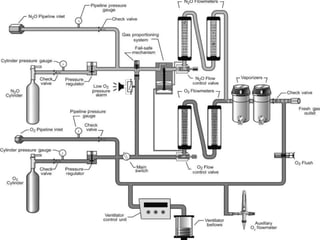
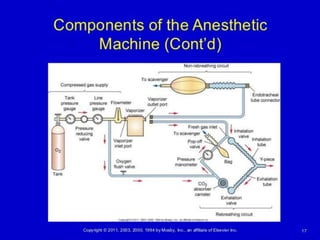
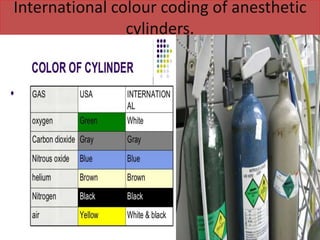
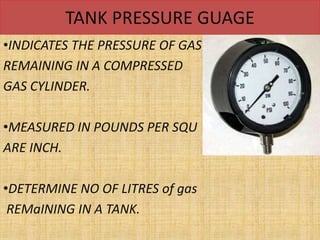
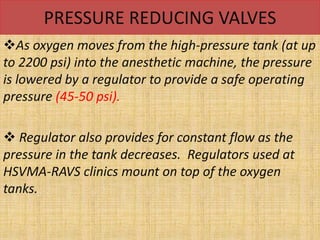
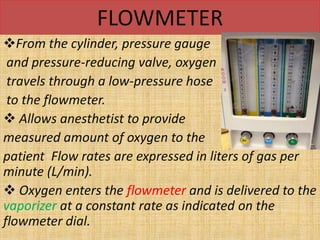
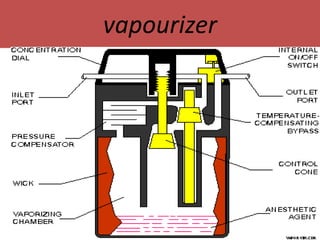
- The main components including gas cylinders, pressure regulators, flowmeters, vaporizers, breathing systems, and absorber canisters.
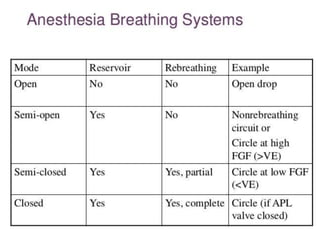
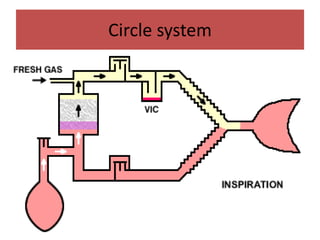
- The differences between rebreathing and non-rebreathing breathing circuits. Rebreathing circuits allow for reuse of exhaled gases while non-rebreathing circuits do not.
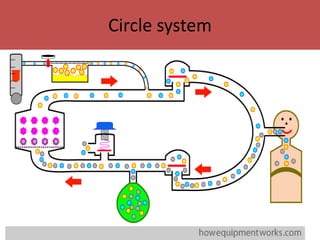
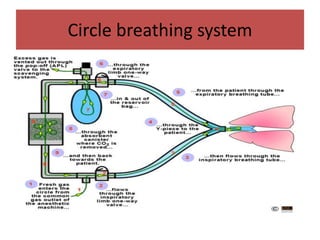
- Key parts like the fresh gas inlet, unidirectional valves, rebreathing bag, and pop-off valve that control gas flow within the breathing system.











































![ANESTHESIA_MACHINE-_PRESSURE_REDUCING_VALVES,_FLOWMETER_AND[1].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/anesthesiamachine-pressurereducingvalvesflowmeterand1-250127121142-c2585726-thumbnail.jpg?width=640&height=640&fit=bounds)



























