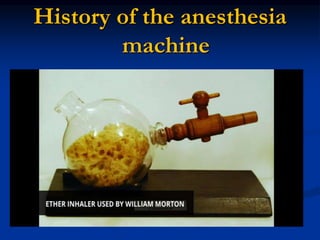
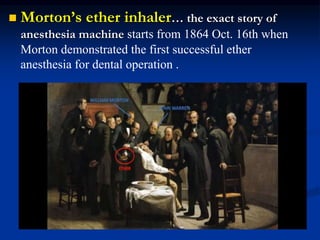
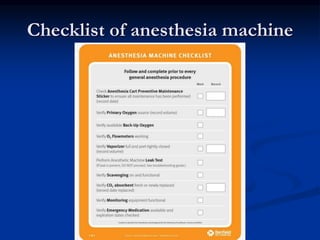
The document provides a history of anesthesia machines and describes their key components and safety features. It discusses how machines have evolved from Morton's ether inhaler in 1864 to modern machines with components like gas delivery systems, ventilators, vaporizers, and monitoring systems. Modern safety features help prevent hypoxic events, ensure minimum oxygen levels, and include vaporizer interlocks and gas connection standards. Regular checklists are important for verifying machine safety and functionality.




















































![ANESTHESIA_MACHINE-_PRESSURE_REDUCING_VALVES,_FLOWMETER_AND[1].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/anesthesiamachine-pressurereducingvalvesflowmeterand1-250127121142-c2585726-thumbnail.jpg?width=640&height=640&fit=bounds)






















