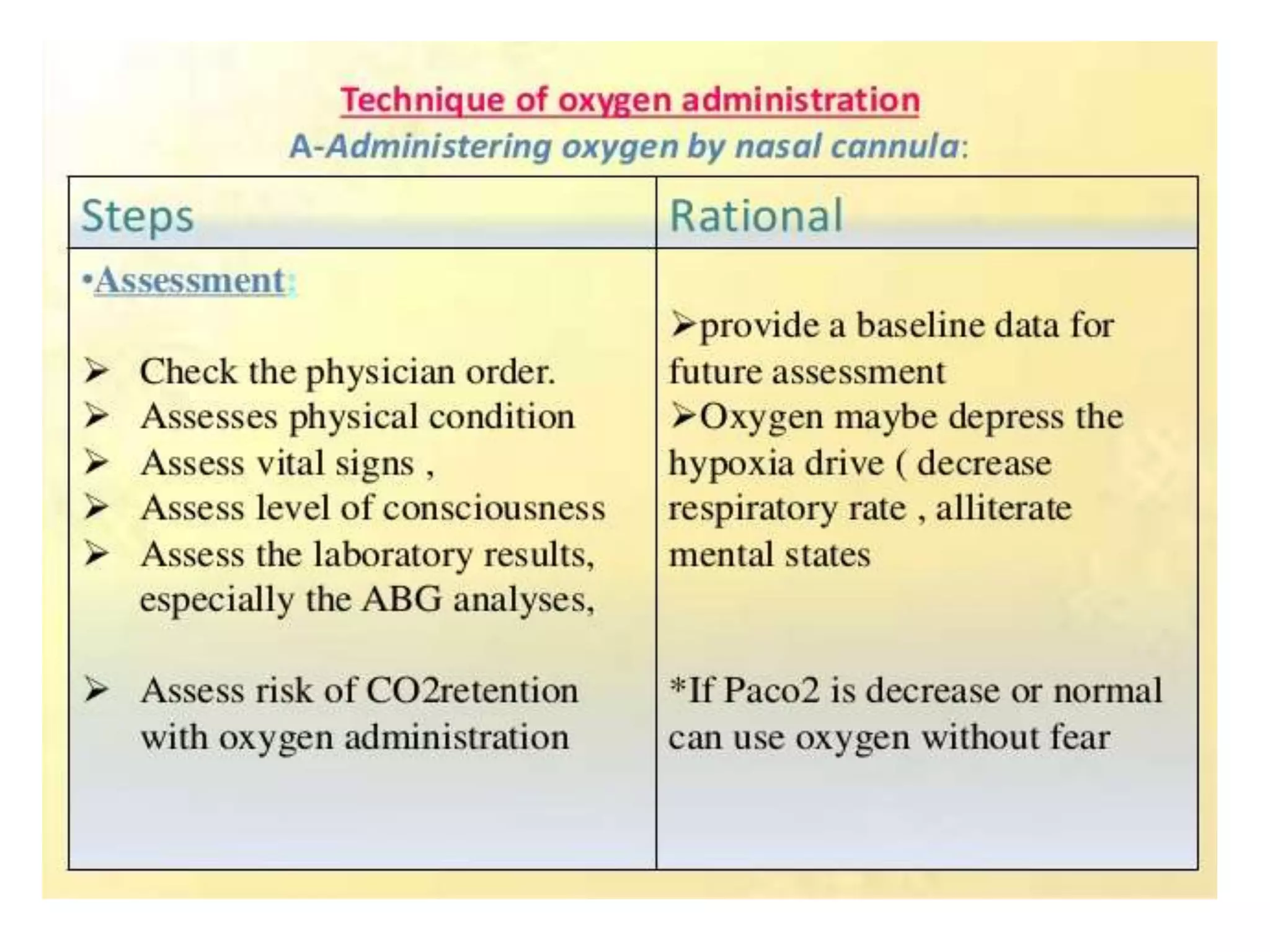
Oxygen therapy involves administering oxygen at concentrations higher than in the air to treat various medical conditions. There are various methods of oxygen delivery including nasal cannulas, face masks, venturi masks, and tents. The goal is to increase oxygen saturation levels in the blood. Potential complications include oxygen toxicity if delivered at too high of a concentration for too long. Precautions must also be taken due to the flammability of oxygen.


![Safety Precautions for Oxygen
Administration
Oxygen is a highly combustible gas.
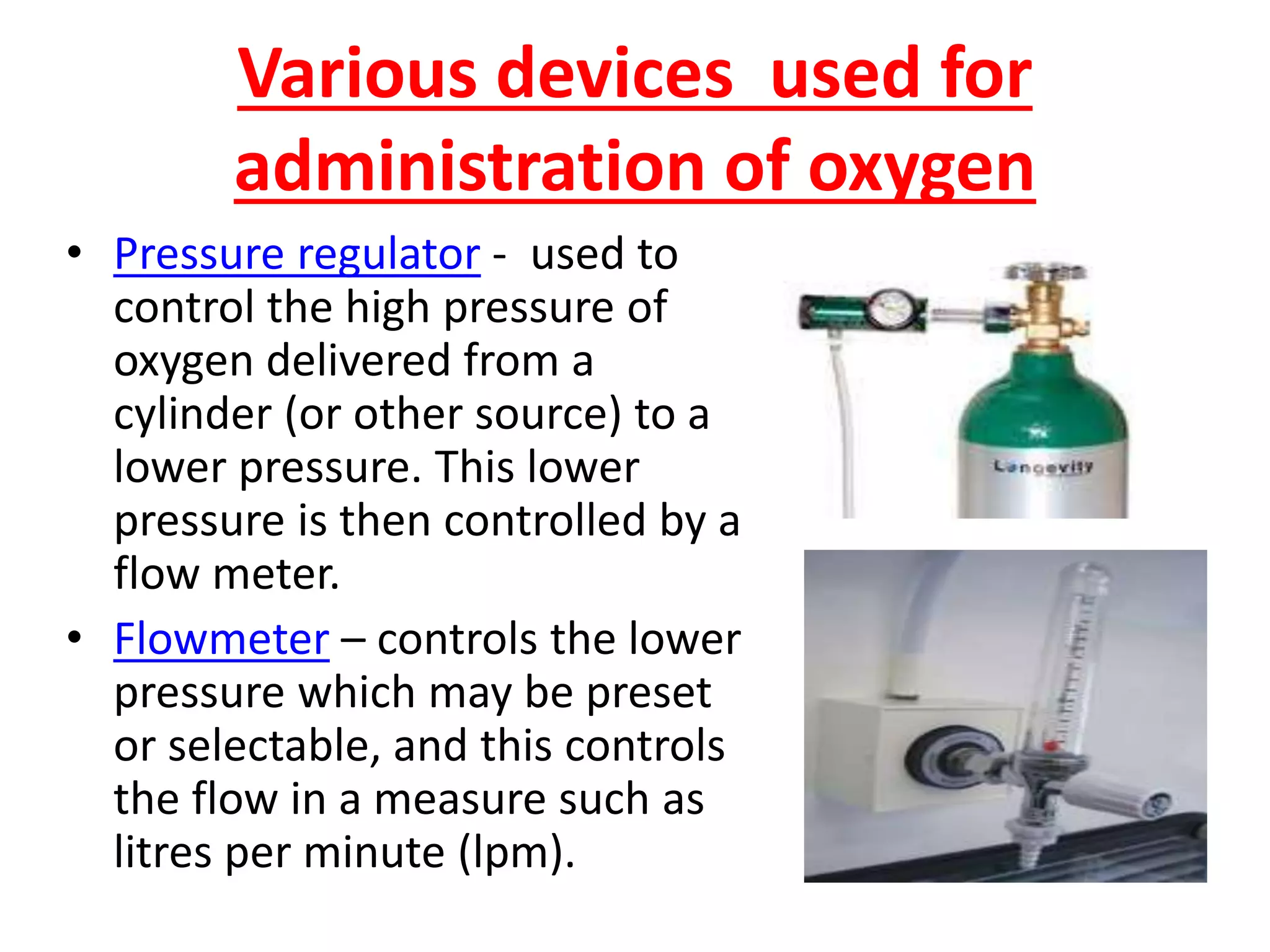
Oxygen is a therapeutic gas and must be prescribed and
adjusted only with a health care provider’s order
Keep oxygen deliver systems 10 feet away from any
open flames.
Keep cylinder always upright position, while
administering secure them to avoid falling.
Check the cylinder for sufficient to administer client
Teach family members to smoke only outside away
from the client and oxygen equipment.
Set up “No Smoking: and “oxygen in Use” signs at the
site of administration and at the door,[ even in home]
according to agency policy.](https://image.slidesharecdn.com/pptonoxygenadministration-200426054900/75/Ppt-on-oxygen-administration-13-2048.jpg)
![Classification of Oxygen
Delivery Systems
• Low flow systems
– Contribute partially to inspired gas client breathes
– Do not provide constant Fio2[fraction /percentage
of inspired oxygen]
– Ex: nasal cannula, simple mask , non-re breather
mask , Partial rebreather mask
• High flow systems
– Deliver specific and constant percent of oxygen
independent of client’s breathing
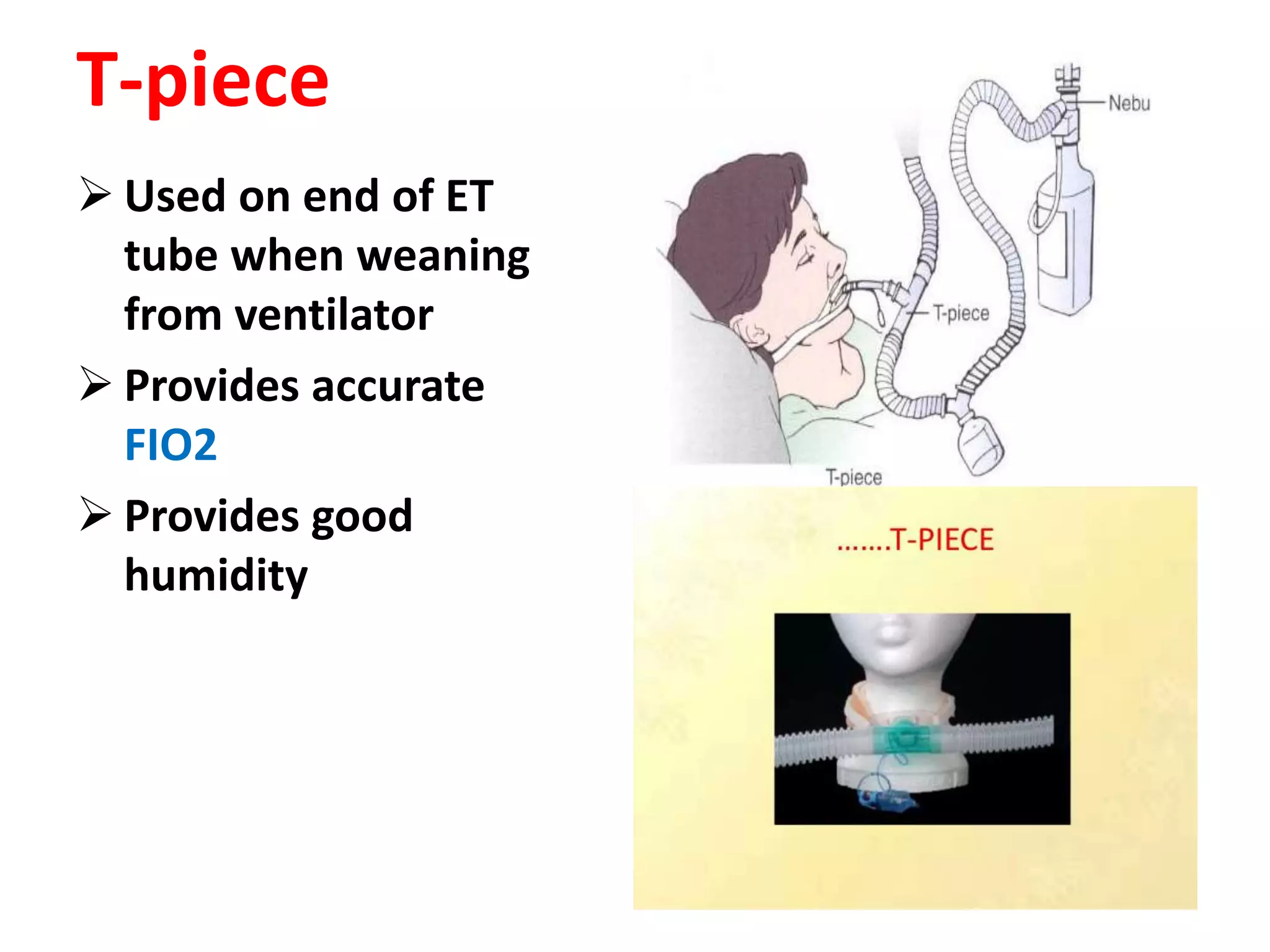
– Ex: Venturi mask,, trach collar, T-piece](https://image.slidesharecdn.com/pptonoxygenadministration-200426054900/75/Ppt-on-oxygen-administration-21-2048.jpg)
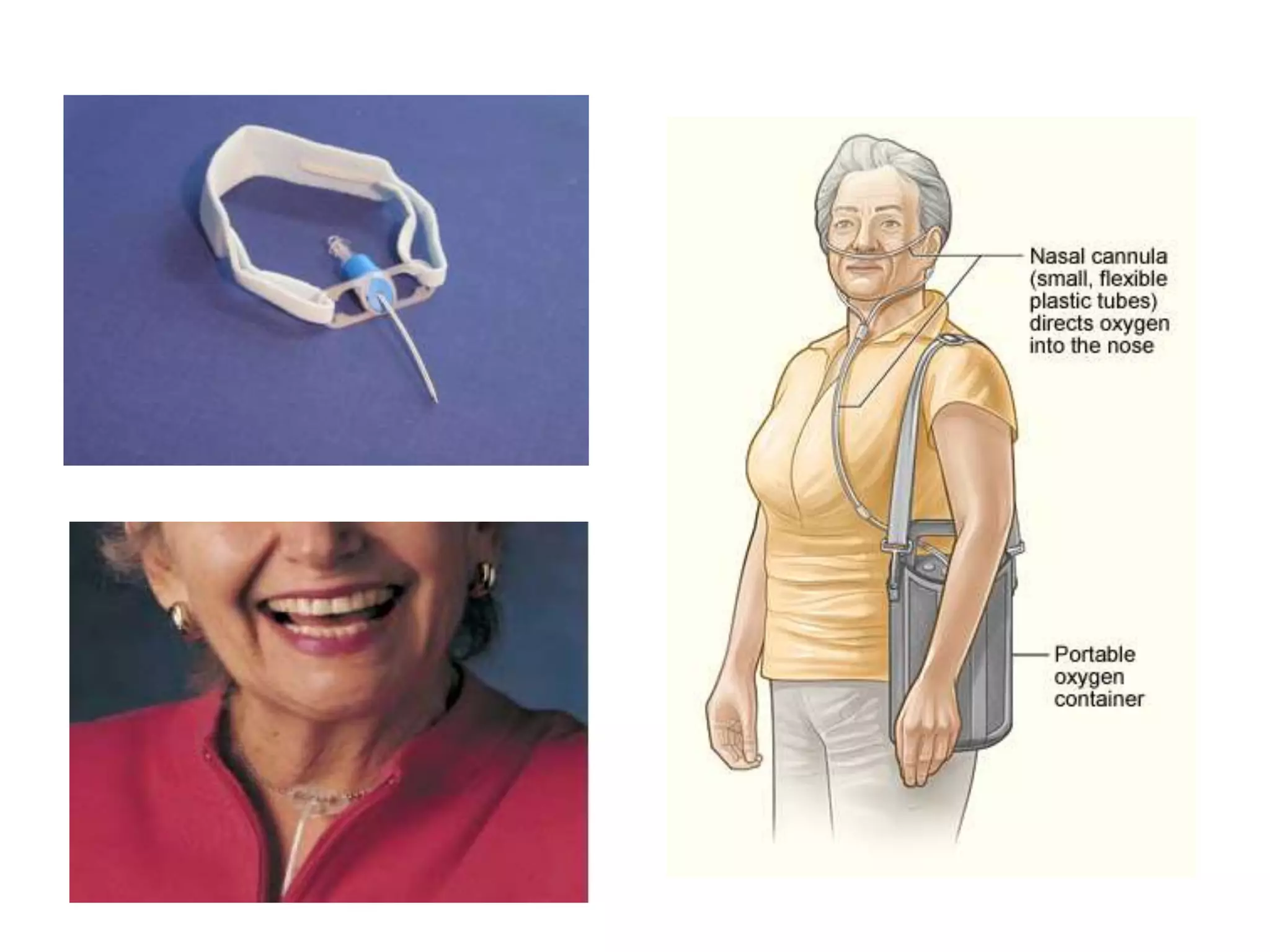
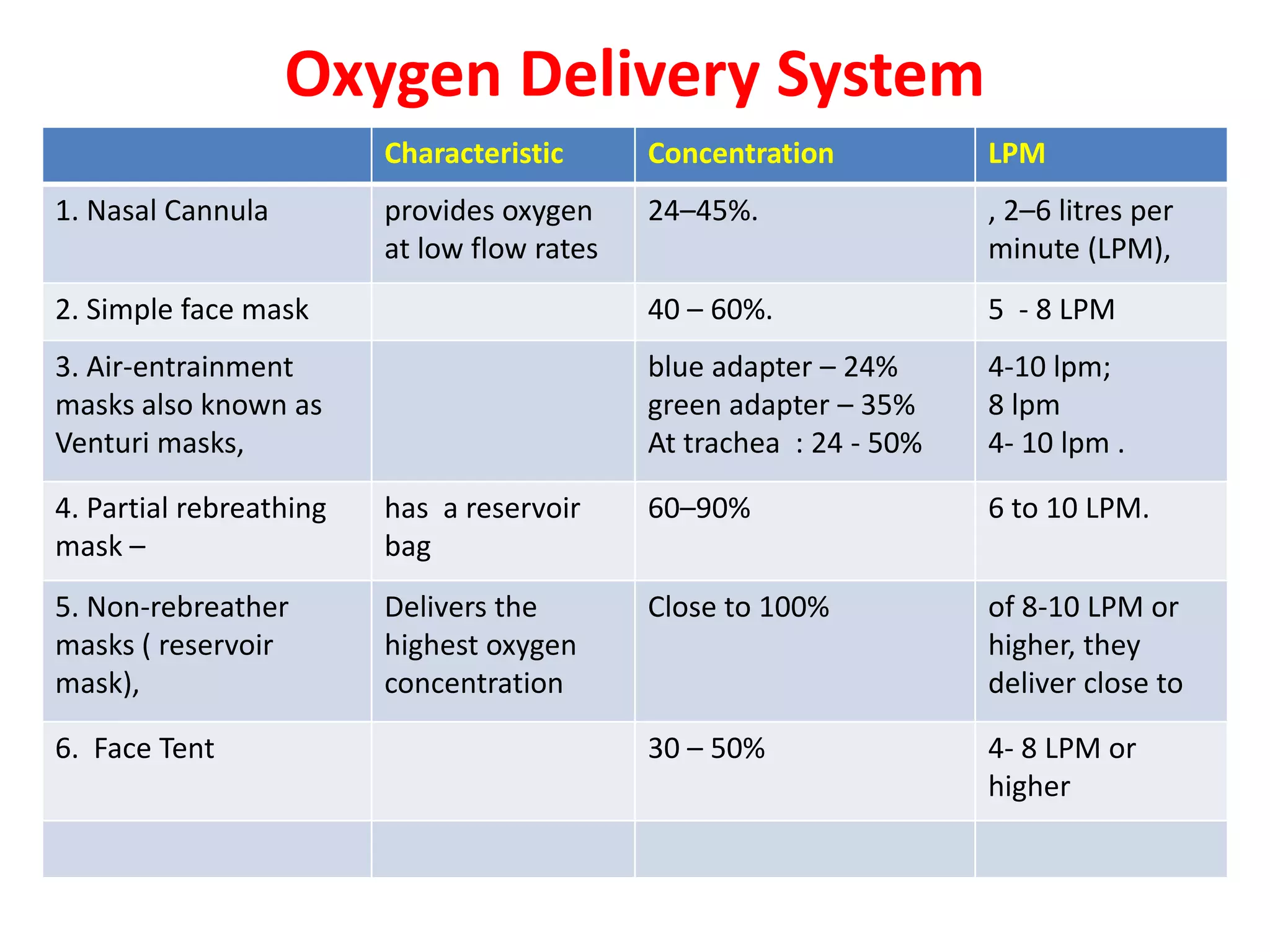
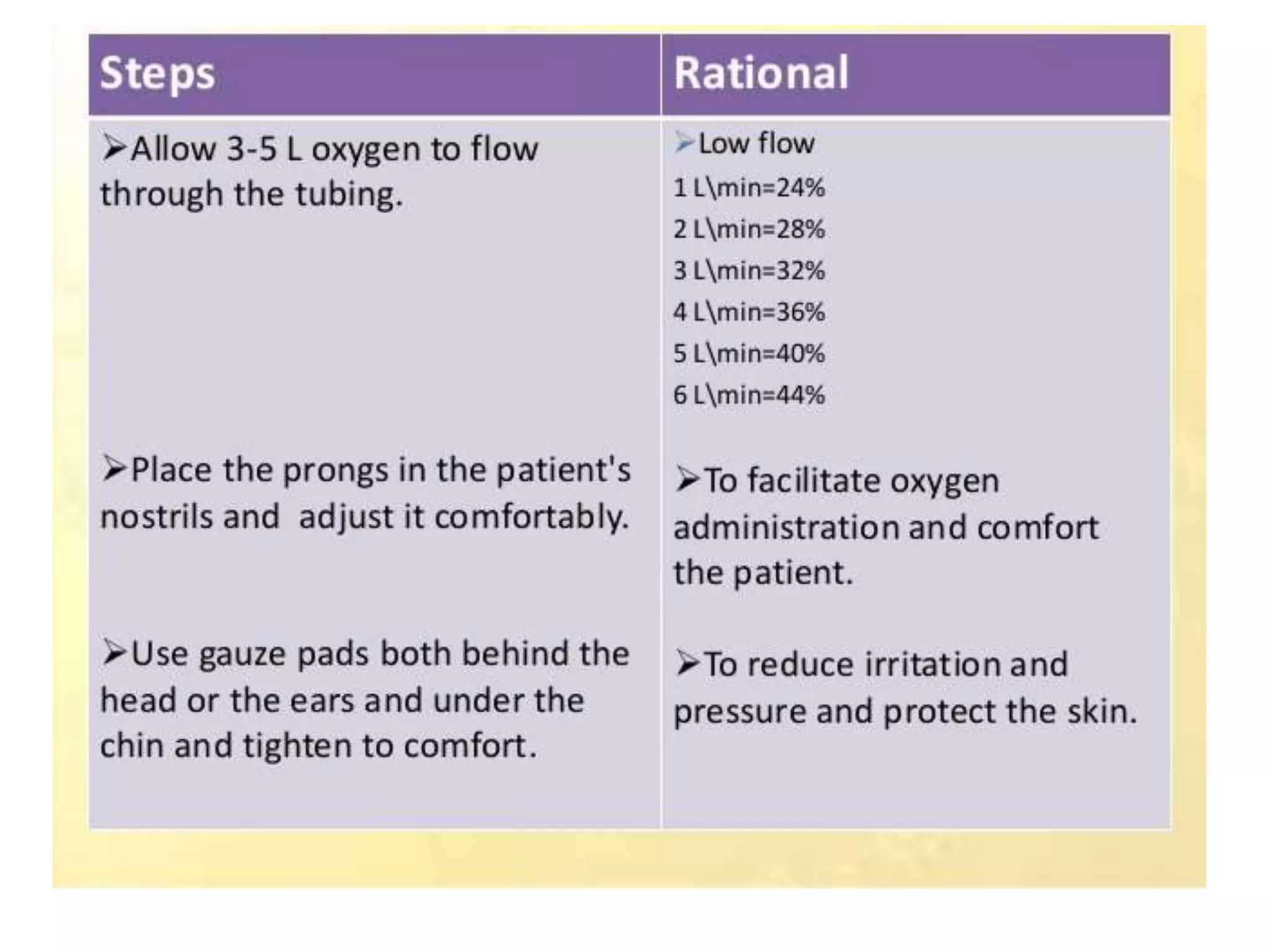
![Nasal cannula(NC)
• is a thin tube with two small nozzles that
protrude into the patient's nostrils.
• Most common and inexpensive device
• provides oxygen at low flow rates, 2–6
liters per minute (LPM), delivering a
concentration of 24–45%.
• allows the patient to continue to talk, eat
and drink while still receiving the
therapy. [home set up]
• associated with greater overall safe ,
comfort, and improved oxygenation and
respiratory rates than with face mask
oxygen.](https://image.slidesharecdn.com/pptonoxygenadministration-200426054900/75/Ppt-on-oxygen-administration-22-2048.jpg)
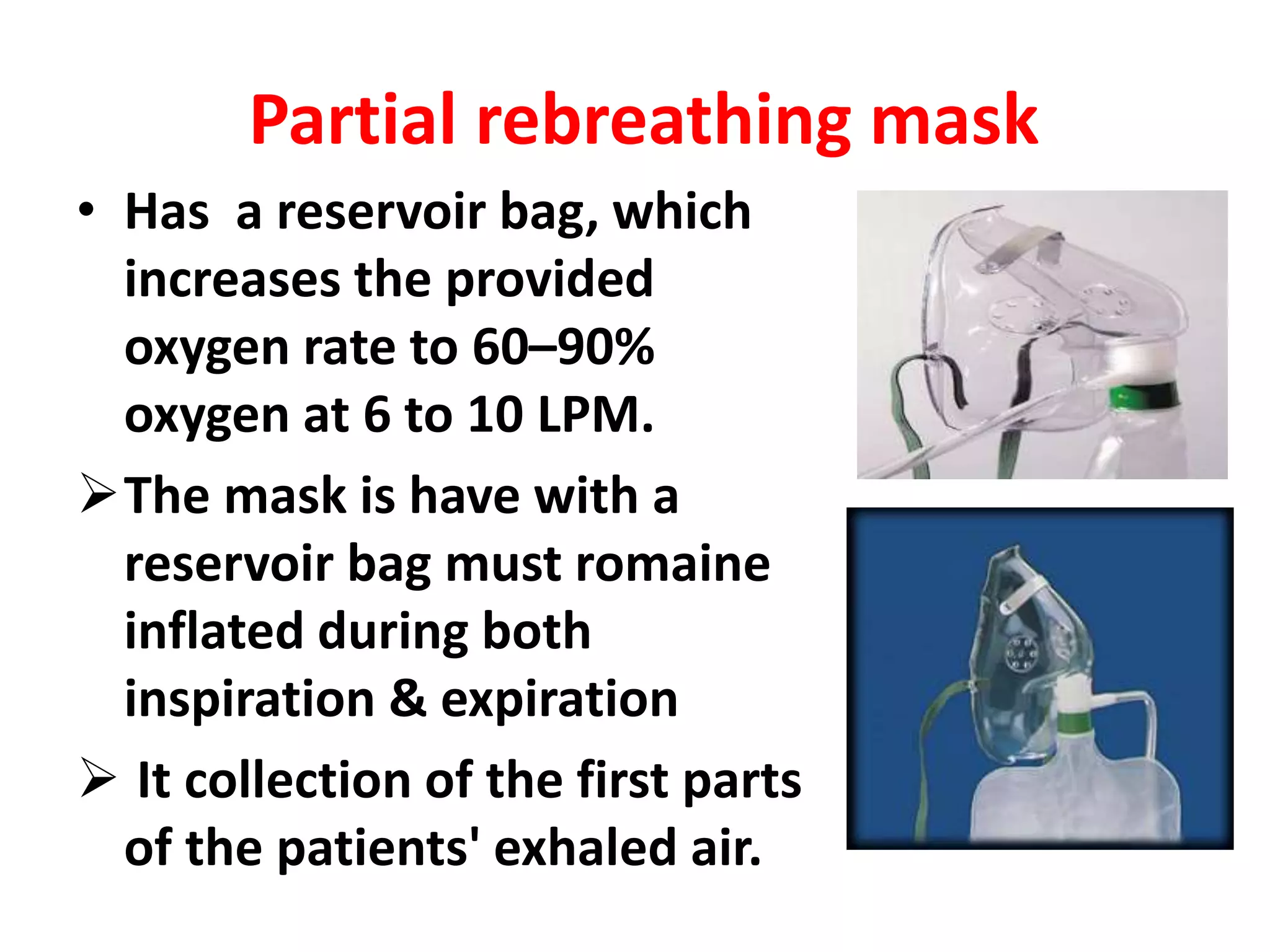
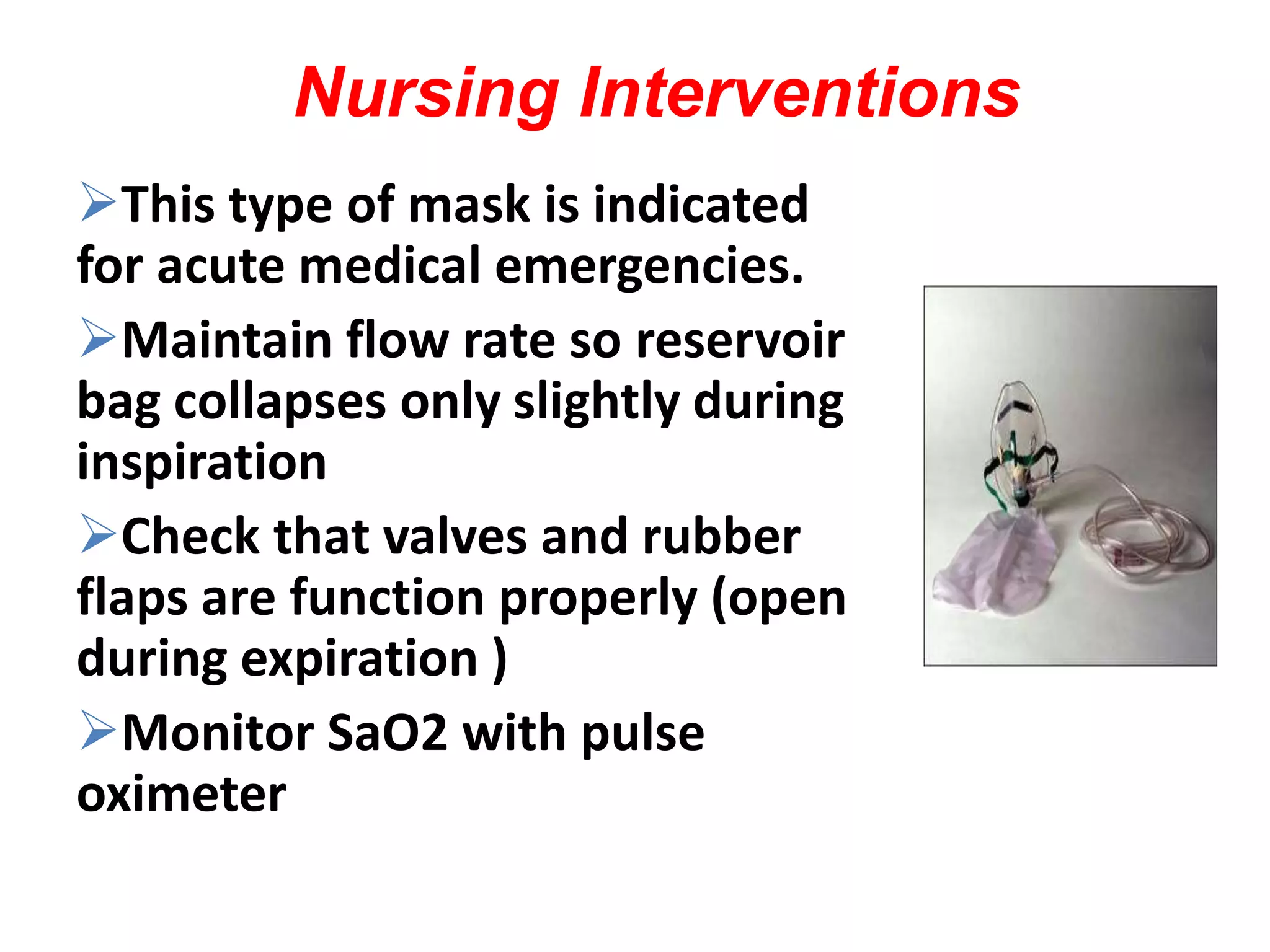
![The non rebreather mask
It is similar to the partial
rebreather mask except two, one
way valve present.
When the patient exhales air. the
one-way valve closes and all of the
expired air is deposited into the
atmosphere, not the reservoir bag.
In this way, the patient is not
rebreathing any of the expired gas.
This mask provides the highest
concentration of oxygen [95-100%]
at a flow rate 6-15 L/min](https://image.slidesharecdn.com/pptonoxygenadministration-200426054900/75/Ppt-on-oxygen-administration-29-2048.jpg)
![Venturi masks [Air-entrainment masks]
Has a wide bore tubing and color
coded jet adapters ( blue adapter –
24% at 4-10 L/ m; green adapter –
35% at 8 lpm)
The mask is so constructed that there
is a constant flow of room air blended
with a fixed concentration of oxygen
can accurately deliver a
predetermined oxygen concentration
to the trachea up to 24 - 50% at 4- 10
L/m .
Each color code corresponds to a
precise oxygen concentration and a
specific liter flow.](https://image.slidesharecdn.com/pptonoxygenadministration-200426054900/75/Ppt-on-oxygen-administration-31-2048.jpg)



















































![2nd yr bsc[n] cet ppt-methods of teaching -nsg education](https://cdn.slidesharecdn.com/ss_thumbnails/2ndyrbscncet-ppt-methodsofteaching-nsgeducation-200426055039-thumbnail.jpg?width=640&height=640&fit=bounds)
















![Apporach to lung biopsy [Auto-saved].pptx latest](https://cdn.slidesharecdn.com/ss_thumbnails/apporachtolungbiopsyauto-saved-251211225655-93258539-thumbnail.jpg?width=640&height=640&fit=bounds)













