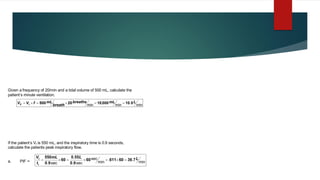
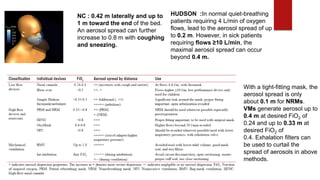
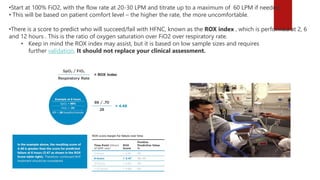
* Vt = 550 mL
* Inspiratory time (Ti) = 0.9 seconds
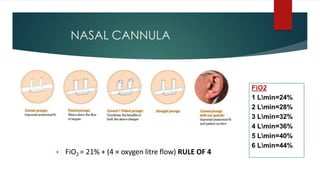
* To calculate peak inspiratory flow (PIF) in L/min:
PIF (L/min) = Vt (mL) / Ti (seconds) * 60
* PIF = 550 mL / 0.9 seconds * 60
* PIF = 61.1 L/min
Therefore, the patient's peak inspiratory flow is 61.1 L/min.






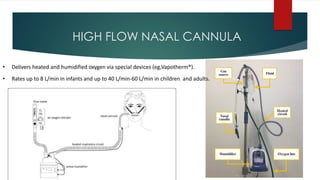
![ Aerosol generation
By increasing the flows from 10 L/min to 60 L/min, HFNC has shown to increase aerosol spread
from 65 to 172 mm in the sagittal plane. It can also cause air leakage around the mask up to 620
mm.[19] Some recommend avoiding the use of HFNC.[20] Aerosol dispersion can be lessened using
a surgical mask and asking patients to breathe through nose with mouth closed.[17] In a human
patient-simulator model, use of a surgical mask during normal cough reduced aerosol spread from
68 cm to 30 cm, and further reduction of diffusion distance was noted with the use of N95 mask.[8]
Recommendation
HFNC can be used to provide oxygen, preferably in patients with acute respiratory failure with P/F
ratio ≥200 mm Hg. It should be ensured that the nasal reservoir used with HFNC is snugly fit, and
the patients are instructed to wear surgical/N95 masks and breathe nasally. OxyMask should be
used at flows ≤20 L/min.](https://image.slidesharecdn.com/oxygentherapyprinciplesandpracticeshahnaali-210621154327/85/Oxygen-therapy-principles_and_practice-shahna-ali-37-320.jpg)