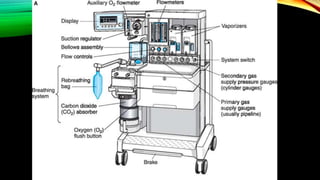
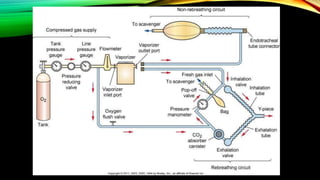
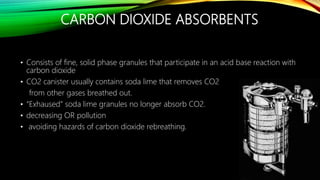
The document describes the key components and functions of an anesthesia machine. It discusses how the machine provides oxygen, removes carbon dioxide, delivers anesthetic agents, and monitors patient safety. The main parts include gas delivery systems from cylinders or pipelines, vaporizers, breathing circuits, carbon dioxide absorbers, and safety features. The goals of the machine are to ventilate the patient, provide supplemental oxygen, deliver anesthetic agents, and monitor for hazards through features like oxygen failure alarms and capnography.






































































![ANESTHESIA_MACHINE-_PRESSURE_REDUCING_VALVES,_FLOWMETER_AND[1].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/anesthesiamachine-pressurereducingvalvesflowmeterand1-250127121142-c2585726-thumbnail.jpg?width=640&height=640&fit=bounds)


































