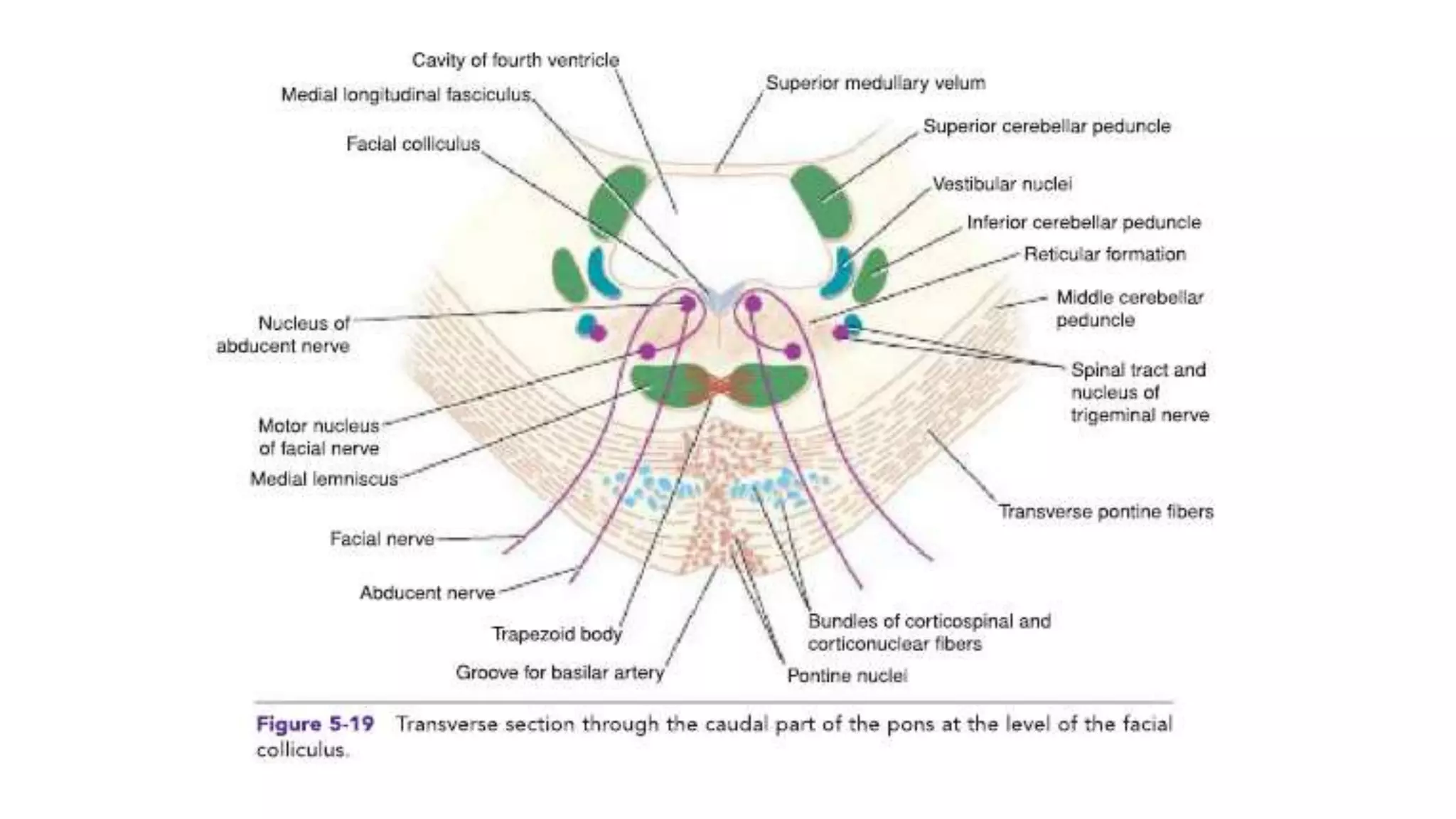
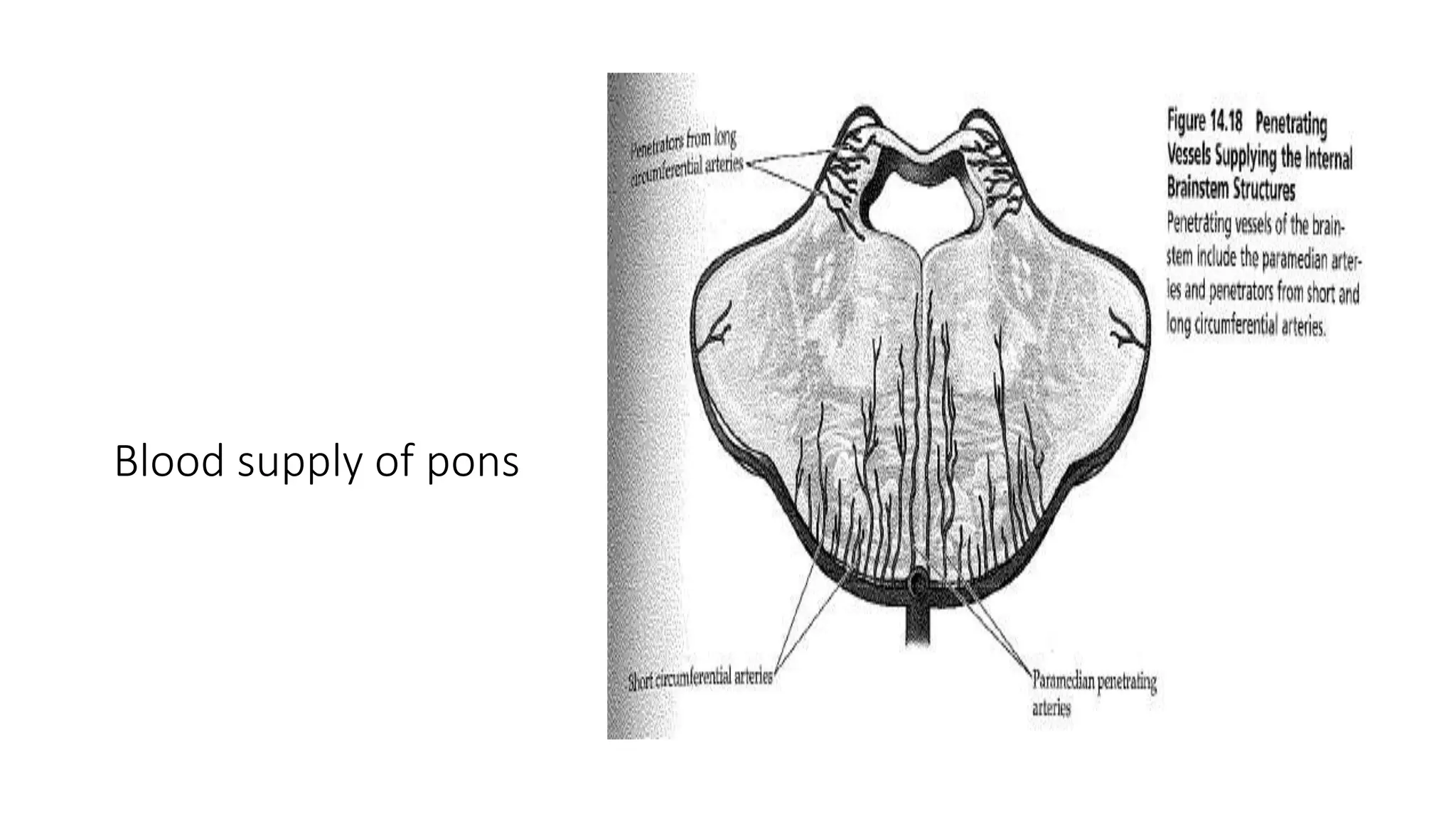
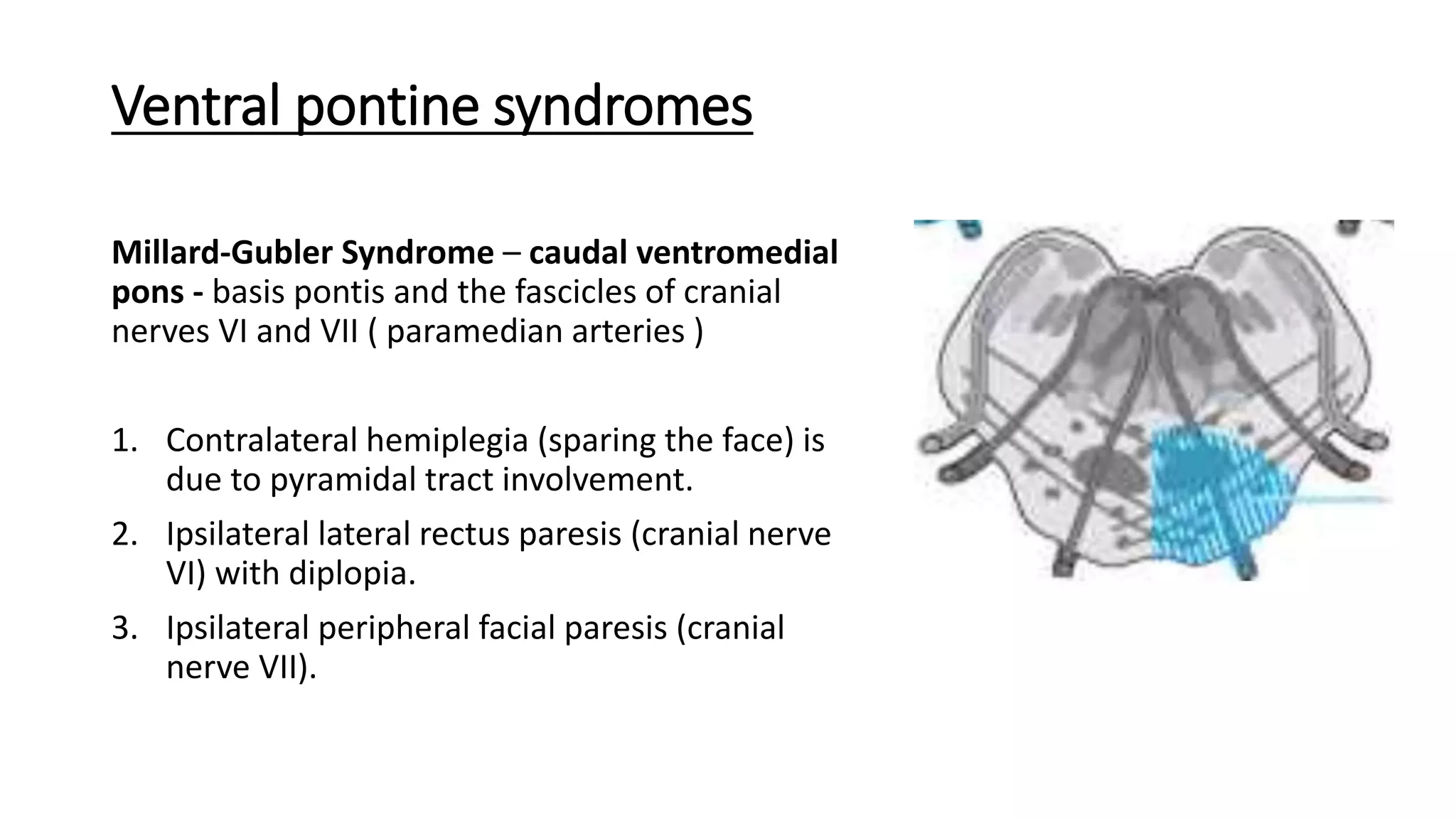
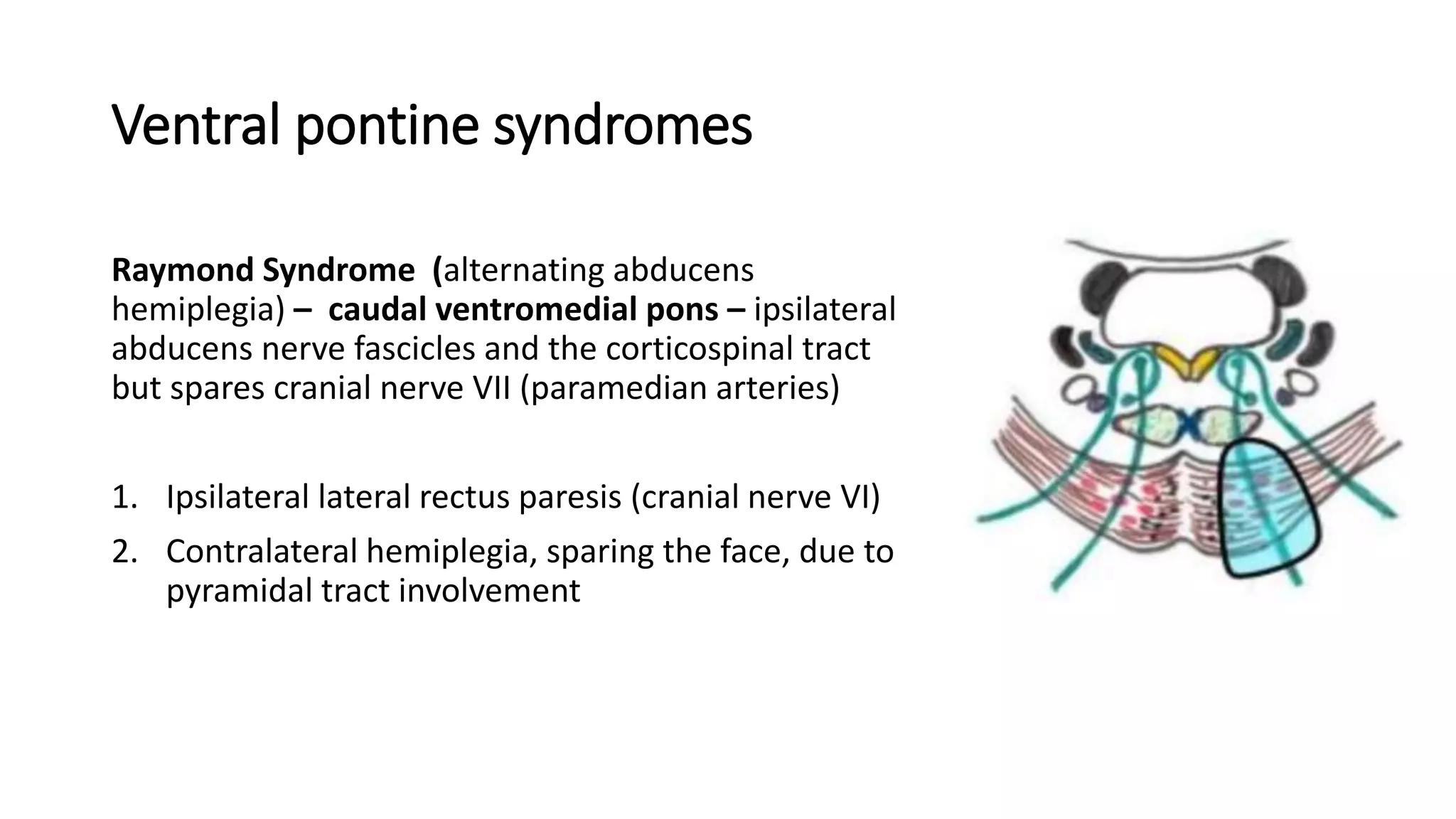
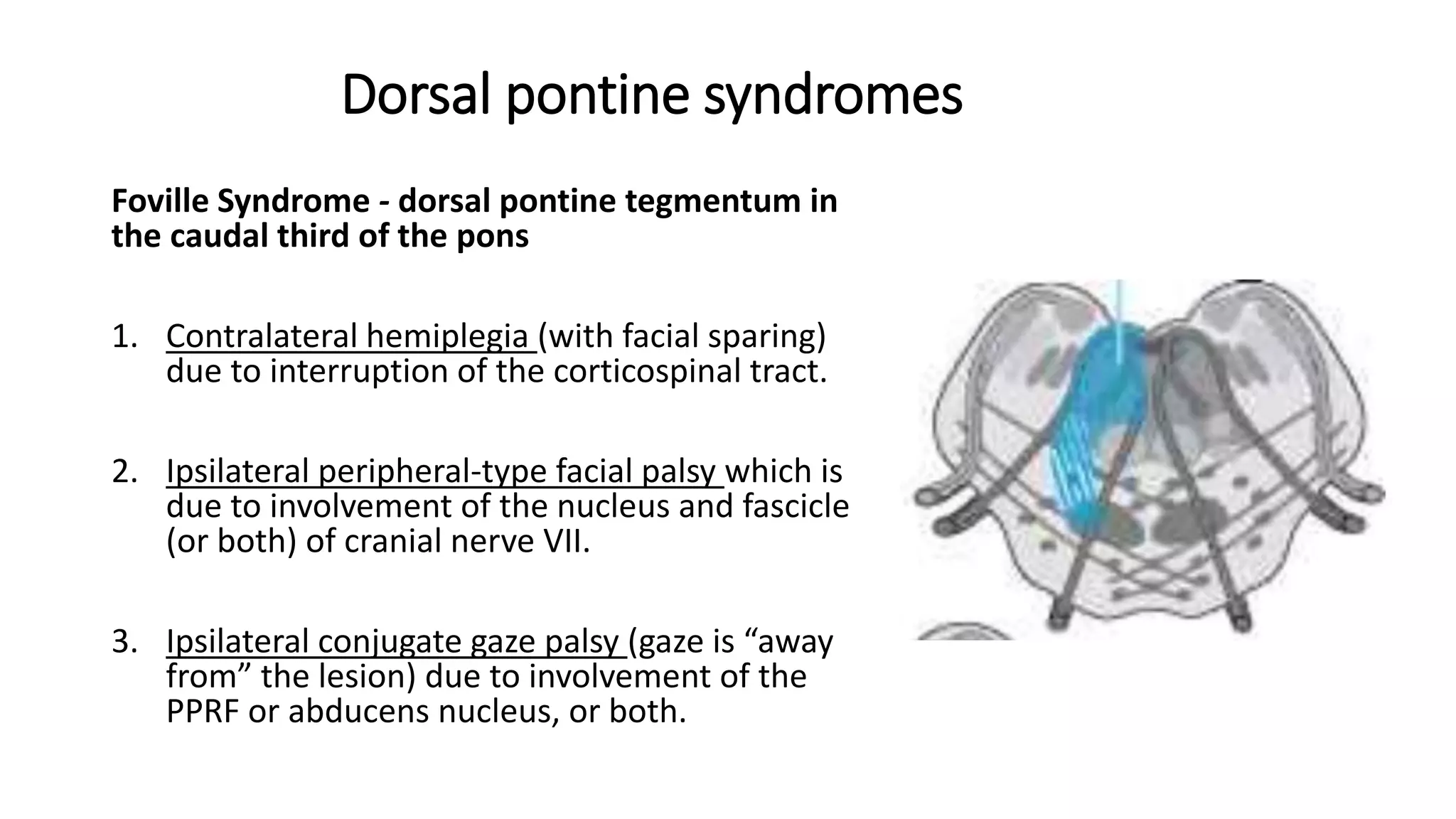
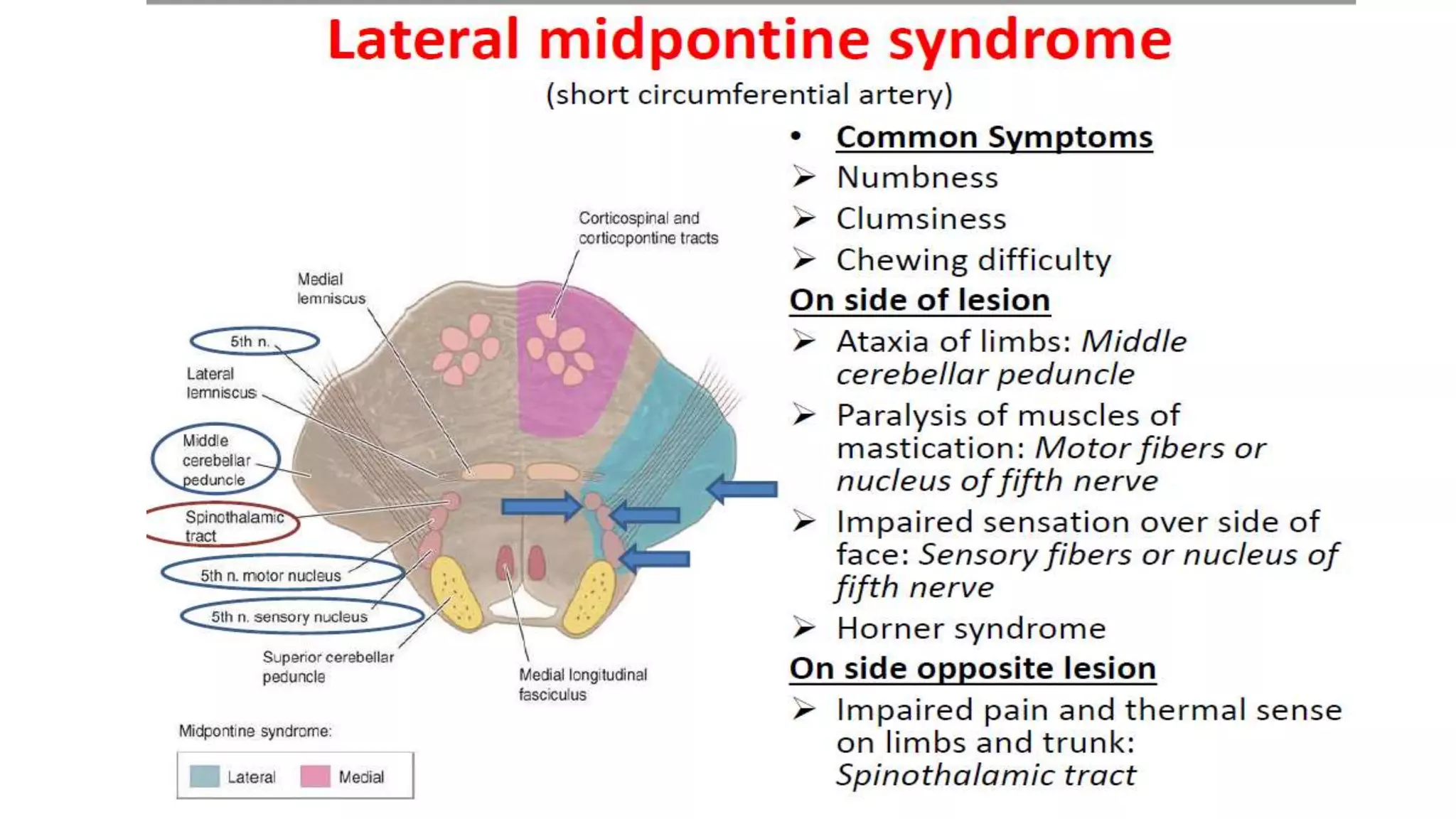
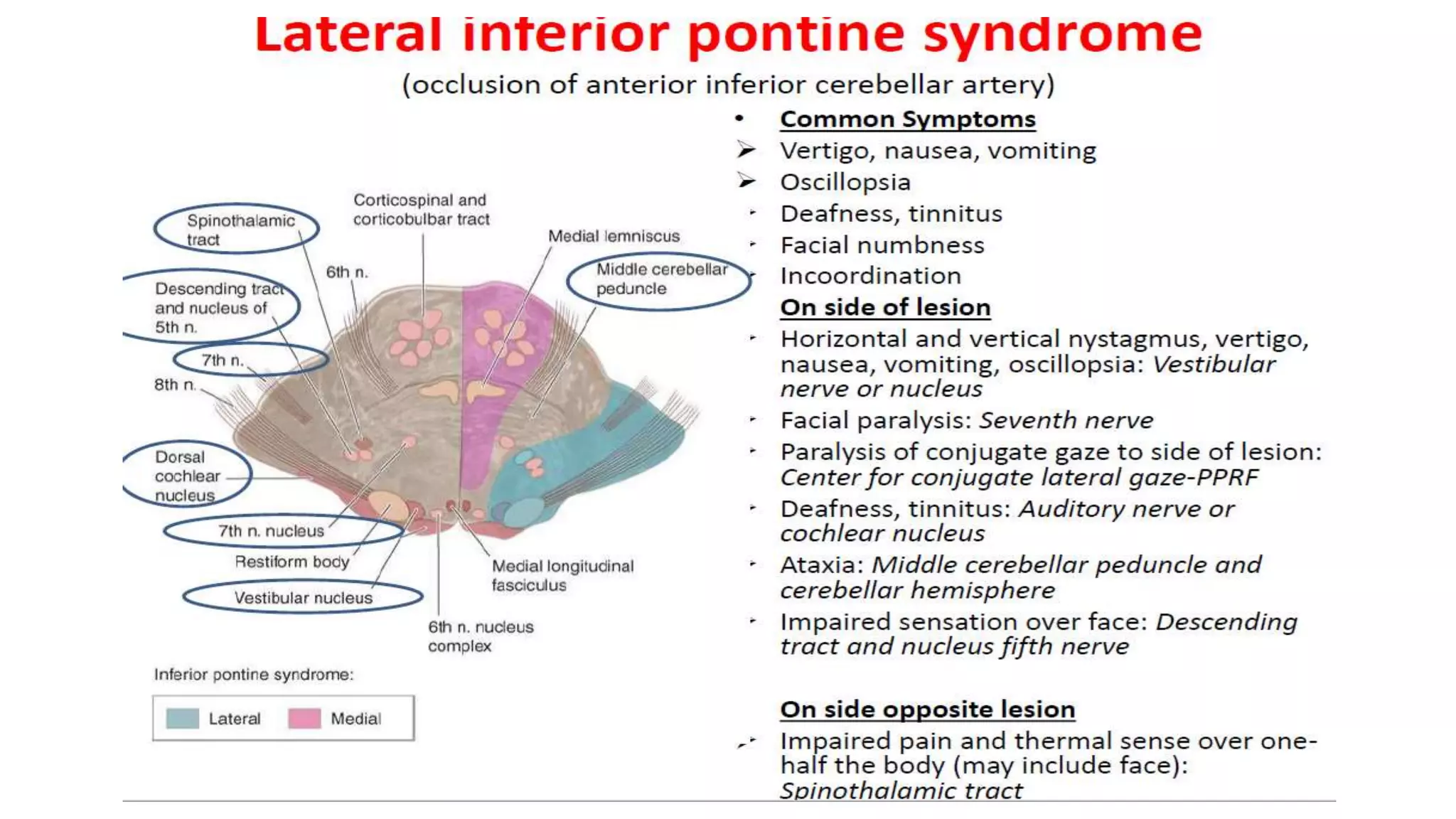
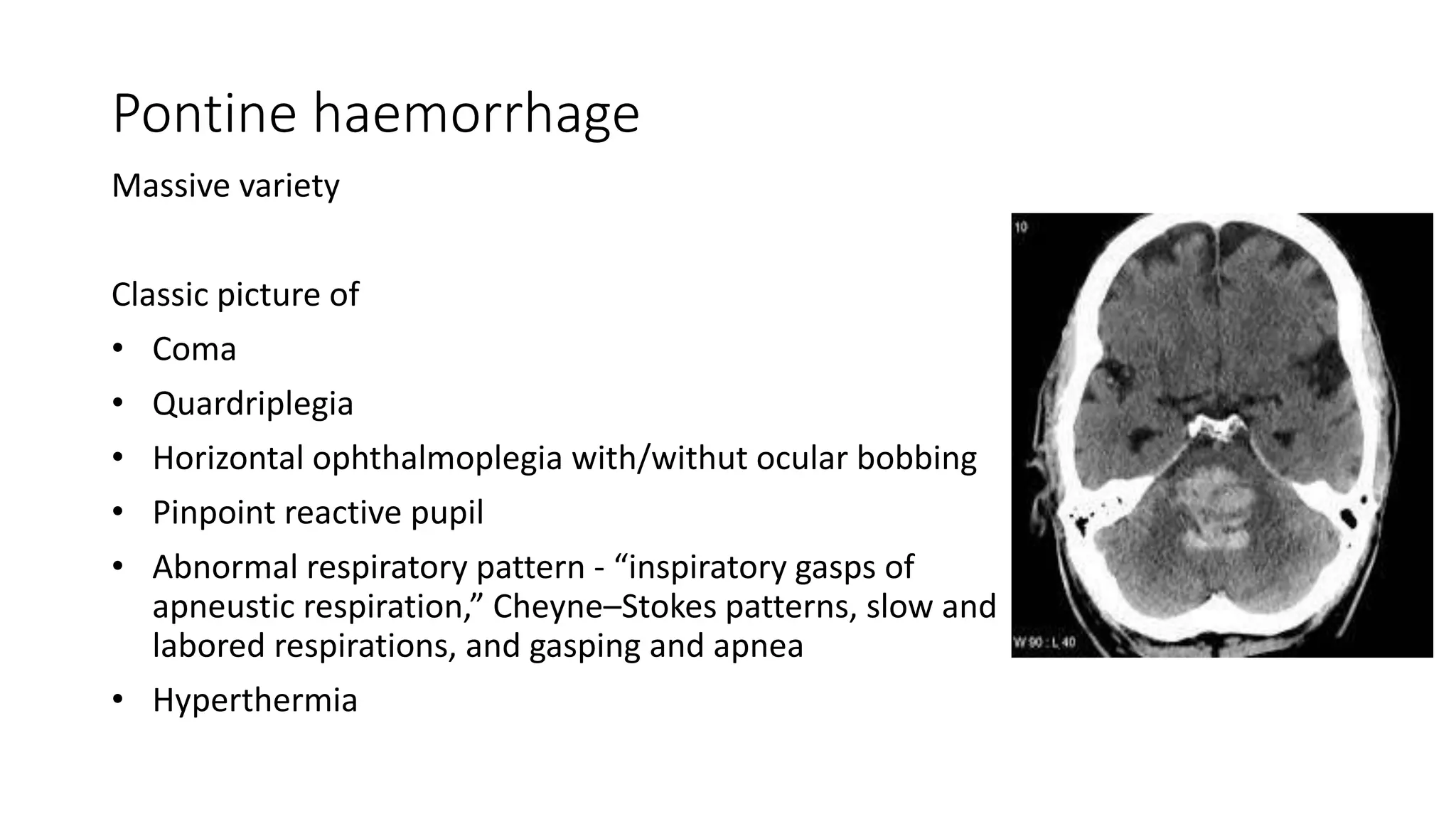
This document summarizes the anatomy and vascular supply of the pons and describes various clinical syndromes that can result from lesions in different regions of the pons. It discusses the tracts that pass through the pons, outlines the vascular territories supplied by different arteries, and describes symptoms associated with medial, lateral, ventral and dorsal pontine lesions. Specific syndromes described include Millard-Gubler syndrome, Raymond syndrome, ataxic hemiparesis, Foville syndrome, and Marie-Foix syndrome. Pontine hemorrhage presentations are also briefly outlined.


























































![DUAL AND TRIPLE ANTITHROMBOTIC THERAPY FOR SECONDARY STROKE [Autosaved].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/dualandtripleantithrombotictherapyforsecondarystrokeautosaved-230904113552-c3502b37-thumbnail.jpg?width=640&height=640&fit=bounds)

































