Downloaded 589 times
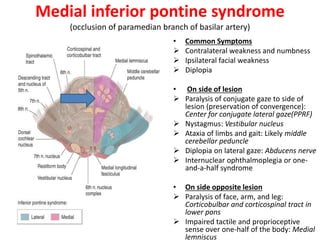
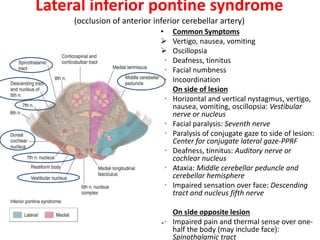
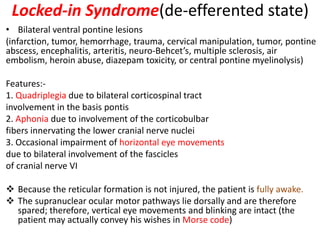
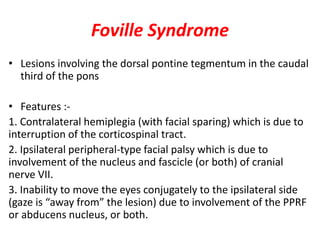
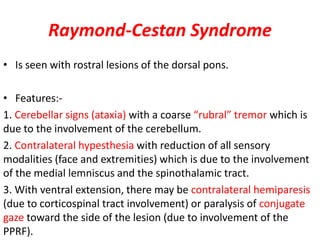


The document provides a detailed anatomical and functional overview of the pons, highlighting its structural divisions, cranial nerve nuclei, and associated pathways. It covers the implications of various pontine syndromes, including their causes, symptoms, and distinguishing features. Conditions such as Millard-Gubler syndrome and locked-in syndrome are specifically mentioned, illustrating the clinical significance of pontine lesions.
































































![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)








