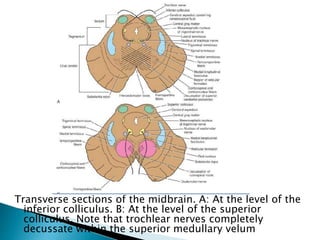
The document discusses various syndromes associated with lesions in different areas of the brainstem. It describes syndromes related to lesions of the posterior cerebral artery including Dejerine-Roussy syndrome and Claude's syndrome. It also summarizes syndromes caused by lesions in specific areas of the pons including the basis pontis, ventral pons, dorsal pons, and ventral medial pons. Syndromes involving the medulla are also outlined such as Wallenberg's lateral medullary syndrome and medial medullary syndrome. Finally, it provides an overview of the anatomy and blood supply of the midbrain and medulla.