Downloaded 171 times

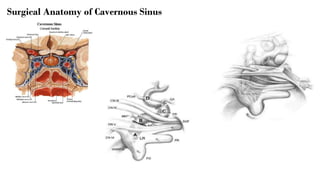

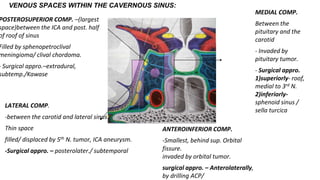
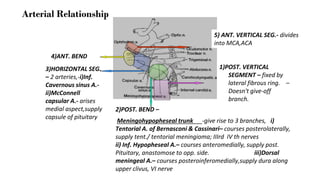
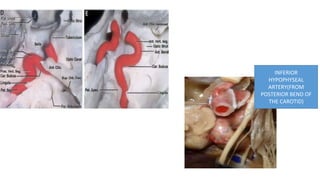
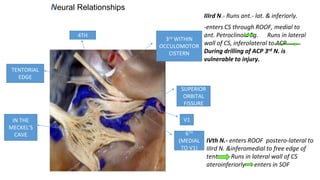


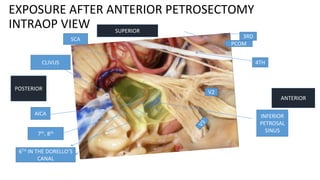
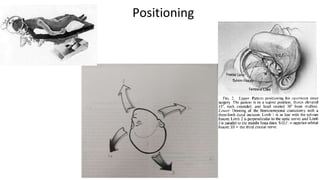

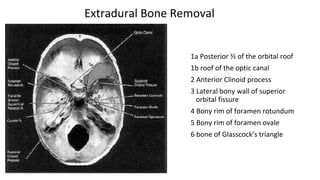
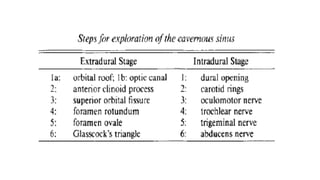
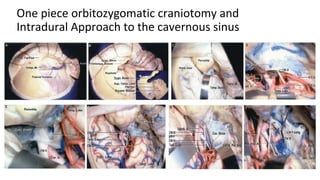
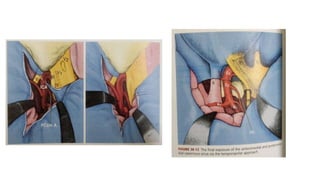
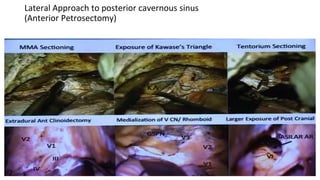
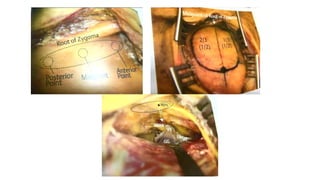
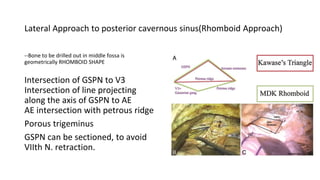
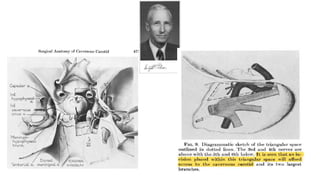




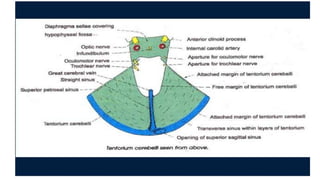
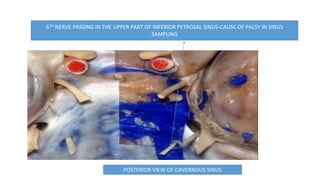

This document discusses the anatomy and surgical approaches to the cavernous sinus region. It begins with a detailed overview of the surgical anatomy, including bony, dural, venous, neural, and arterial relationships. It then describes several surgical approaches to the cavernous sinus, including the pterional craniotomy with extradural and intradural approaches, anterolateral temporopolar transcavernous approaches, lateral approaches to the posterior cavernous sinus, and extended middle fossa approaches. Technical considerations for tumor resection and hemostasis within the cavernous sinus are also reviewed.

























































![谷歌留痕技术 [ 𝙩𝙤𝙥 𝟮𝟯𝟯. 𝙘 𝙤𝙢 ]](https://cdn.slidesharecdn.com/ss_thumbnails/top233-260130174328-3833018c-thumbnail.jpg?width=640&height=640&fit=bounds)









