The urinary system consists of the kidneys, ureters, urinary bladder, and urethra. The kidneys filter waste from the blood to produce urine. The urine passes from the kidneys to the bladder via the ureters. The bladder stores urine until micturition. The urethra then carries urine out of the body. The urinary system regulates water balance and the levels of electrolytes, acids, and bases in the blood to maintain homeostasis. Nephrons are the functional units of the kidneys that filter blood and form urine through processes like filtration, reabsorption, and secretion.
Blood is carried through the body via blood vessels. An artery is a blood vessel that carries blood away from the heart, where it branches into ever-smaller vessels.
The blood vessels are the components of the circulatory system that transport blood throughout the human body. These vessels transport blood cells, nutrients, and oxygen to the tissues of the body. They also take waste and carbon dioxide away from the tissues.
Skeletal system. anatomy and physiology of skeletal system. appendicular skel...mamtabisht10
SKELETAL SYSTEM
bones, cartilage and ligaments are tightly joined to form a strong, flexible framework called skeletal system
anatomy and physiology of axial and appendicular skeletal system
Axial Skeleton: The axial skeleton includes the skull, spine, ribs and sternum.
Appendicular Skeleton:
The appendicular skeleton includes the appendages of the body, which are the shoulders, arms, hips, and legs.
Blood is carried through the body via blood vessels. An artery is a blood vessel that carries blood away from the heart, where it branches into ever-smaller vessels.
The blood vessels are the components of the circulatory system that transport blood throughout the human body. These vessels transport blood cells, nutrients, and oxygen to the tissues of the body. They also take waste and carbon dioxide away from the tissues.
Skeletal system. anatomy and physiology of skeletal system. appendicular skel...mamtabisht10
SKELETAL SYSTEM
bones, cartilage and ligaments are tightly joined to form a strong, flexible framework called skeletal system
anatomy and physiology of axial and appendicular skeletal system
Axial Skeleton: The axial skeleton includes the skull, spine, ribs and sternum.
Appendicular Skeleton:
The appendicular skeleton includes the appendages of the body, which are the shoulders, arms, hips, and legs.
Life of every organism depends on certain basic processes. Excretion is one among them. Different organisms follow different modes of excretion. In complex organisms including humans, there is a specialized system for excretion called human excretory system.
The genitourinary system, or urogenital system, are the organs of the reproductive system and the urinary system. These are grouped together because of their proximity to each other, their common embryological origin and the use of common pathways, like the male urethra.
Report Back from SGO 2024: What’s the Latest in Cervical Cancer?bkling
Are you curious about what’s new in cervical cancer research or unsure what the findings mean? Join Dr. Emily Ko, a gynecologic oncologist at Penn Medicine, to learn about the latest updates from the Society of Gynecologic Oncology (SGO) 2024 Annual Meeting on Women’s Cancer. Dr. Ko will discuss what the research presented at the conference means for you and answer your questions about the new developments.
New Directions in Targeted Therapeutic Approaches for Older Adults With Mantl...i3 Health
i3 Health is pleased to make the speaker slides from this activity available for use as a non-accredited self-study or teaching resource.
This slide deck presented by Dr. Kami Maddocks, Professor-Clinical in the Division of Hematology and
Associate Division Director for Ambulatory Operations
The Ohio State University Comprehensive Cancer Center, will provide insight into new directions in targeted therapeutic approaches for older adults with mantle cell lymphoma.
STATEMENT OF NEED
Mantle cell lymphoma (MCL) is a rare, aggressive B-cell non-Hodgkin lymphoma (NHL) accounting for 5% to 7% of all lymphomas. Its prognosis ranges from indolent disease that does not require treatment for years to very aggressive disease, which is associated with poor survival (Silkenstedt et al, 2021). Typically, MCL is diagnosed at advanced stage and in older patients who cannot tolerate intensive therapy (NCCN, 2022). Although recent advances have slightly increased remission rates, recurrence and relapse remain very common, leading to a median overall survival between 3 and 6 years (LLS, 2021). Though there are several effective options, progress is still needed towards establishing an accepted frontline approach for MCL (Castellino et al, 2022). Treatment selection and management of MCL are complicated by the heterogeneity of prognosis, advanced age and comorbidities of patients, and lack of an established standard approach for treatment, making it vital that clinicians be familiar with the latest research and advances in this area. In this activity chaired by Michael Wang, MD, Professor in the Department of Lymphoma & Myeloma at MD Anderson Cancer Center, expert faculty will discuss prognostic factors informing treatment, the promising results of recent trials in new therapeutic approaches, and the implications of treatment resistance in therapeutic selection for MCL.
Target Audience
Hematology/oncology fellows, attending faculty, and other health care professionals involved in the treatment of patients with mantle cell lymphoma (MCL).
Learning Objectives
1.) Identify clinical and biological prognostic factors that can guide treatment decision making for older adults with MCL
2.) Evaluate emerging data on targeted therapeutic approaches for treatment-naive and relapsed/refractory MCL and their applicability to older adults
3.) Assess mechanisms of resistance to targeted therapies for MCL and their implications for treatment selection
Explore natural remedies for syphilis treatment in Singapore. Discover alternative therapies, herbal remedies, and lifestyle changes that may complement conventional treatments. Learn about holistic approaches to managing syphilis symptoms and supporting overall health.
- Video recording of this lecture in English language: https://youtu.be/lK81BzxMqdo
- Video recording of this lecture in Arabic language: https://youtu.be/Ve4P0COk9OI
- Link to download the book free: https://nephrotube.blogspot.com/p/nephrotube-nephrology-books.html
- Link to NephroTube website: www.NephroTube.com
- Link to NephroTube social media accounts: https://nephrotube.blogspot.com/p/join-nephrotube-on-social-media.html
Ethanol (CH3CH2OH), or beverage alcohol, is a two-carbon alcohol
that is rapidly distributed in the body and brain. Ethanol alters many
neurochemical systems and has rewarding and addictive properties. It
is the oldest recreational drug and likely contributes to more morbidity,
mortality, and public health costs than all illicit drugs combined. The
5th edition of the Diagnostic and Statistical Manual of Mental Disorders
(DSM-5) integrates alcohol abuse and alcohol dependence into a single
disorder called alcohol use disorder (AUD), with mild, moderate,
and severe subclassifications (American Psychiatric Association, 2013).
In the DSM-5, all types of substance abuse and dependence have been
combined into a single substance use disorder (SUD) on a continuum
from mild to severe. A diagnosis of AUD requires that at least two of
the 11 DSM-5 behaviors be present within a 12-month period (mild
AUD: 2–3 criteria; moderate AUD: 4–5 criteria; severe AUD: 6–11 criteria).
The four main behavioral effects of AUD are impaired control over
drinking, negative social consequences, risky use, and altered physiological
effects (tolerance, withdrawal). This chapter presents an overview
of the prevalence and harmful consequences of AUD in the U.S.,
the systemic nature of the disease, neurocircuitry and stages of AUD,
comorbidities, fetal alcohol spectrum disorders, genetic risk factors, and
pharmacotherapies for AUD.
TEST BANK for Operations Management, 14th Edition by William J. Stevenson, Ve...kevinkariuki227
TEST BANK for Operations Management, 14th Edition by William J. Stevenson, Verified Chapters 1 - 19, Complete Newest Version.pdf
TEST BANK for Operations Management, 14th Edition by William J. Stevenson, Verified Chapters 1 - 19, Complete Newest Version.pdf
Lung Cancer: Artificial Intelligence, Synergetics, Complex System Analysis, S...Oleg Kshivets
RESULTS: Overall life span (LS) was 2252.1±1742.5 days and cumulative 5-year survival (5YS) reached 73.2%, 10 years – 64.8%, 20 years – 42.5%. 513 LCP lived more than 5 years (LS=3124.6±1525.6 days), 148 LCP – more than 10 years (LS=5054.4±1504.1 days).199 LCP died because of LC (LS=562.7±374.5 days). 5YS of LCP after bi/lobectomies was significantly superior in comparison with LCP after pneumonectomies (78.1% vs.63.7%, P=0.00001 by log-rank test). AT significantly improved 5YS (66.3% vs. 34.8%) (P=0.00000 by log-rank test) only for LCP with N1-2. Cox modeling displayed that 5YS of LCP significantly depended on: phase transition (PT) early-invasive LC in terms of synergetics, PT N0—N12, cell ratio factors (ratio between cancer cells- CC and blood cells subpopulations), G1-3, histology, glucose, AT, blood cell circuit, prothrombin index, heparin tolerance, recalcification time (P=0.000-0.038). Neural networks, genetic algorithm selection and bootstrap simulation revealed relationships between 5YS and PT early-invasive LC (rank=1), PT N0—N12 (rank=2), thrombocytes/CC (3), erythrocytes/CC (4), eosinophils/CC (5), healthy cells/CC (6), lymphocytes/CC (7), segmented neutrophils/CC (8), stick neutrophils/CC (9), monocytes/CC (10); leucocytes/CC (11). Correct prediction of 5YS was 100% by neural networks computing (area under ROC curve=1.0; error=0.0).
CONCLUSIONS: 5YS of LCP after radical procedures significantly depended on: 1) PT early-invasive cancer; 2) PT N0--N12; 3) cell ratio factors; 4) blood cell circuit; 5) biochemical factors; 6) hemostasis system; 7) AT; 8) LC characteristics; 9) LC cell dynamics; 10) surgery type: lobectomy/pneumonectomy; 11) anthropometric data. Optimal diagnosis and treatment strategies for LC are: 1) screening and early detection of LC; 2) availability of experienced thoracic surgeons because of complexity of radical procedures; 3) aggressive en block surgery and adequate lymph node dissection for completeness; 4) precise prediction; 5) adjuvant chemoimmunoradiotherapy for LCP with unfavorable prognosis.
micro teaching on communication m.sc nursing.pdfAnurag Sharma
Microteaching is a unique model of practice teaching. It is a viable instrument for the. desired change in the teaching behavior or the behavior potential which, in specified types of real. classroom situations, tends to facilitate the achievement of specified types of objectives.
2. ORGANS OF THE URINARY SYSTEM
Kidneys
Ureters
Urinary bladder
Urethra
Figure 15.1a
3. FUNCTIONS OF THE URINARY SYSTEM
Elimination of waste
products
Nitrogenous
wastes
Toxins
Drugs
Regulate aspects of
homeostasis
Water balance
Electrolytes
Acid-base balance
Blood pressure
RBC production
Activation of vit.D
4. LOCATION OF THE KIDNEYS
Against the dorsal body wall
At the level of T12 to L3
The right kidney is slightly lower than the left
Attached to ureters, renal blood vessels, and nerves at
renal hilus
Atop each kidney is an adrenal gland
5. COVERINGS OF THE KIDNEYS
Renal capsule
Surrounds each kidney
Adipose capsule
Surrounds the kidney
Provides protection to the kidney
Helps keep the kidney in its correct location
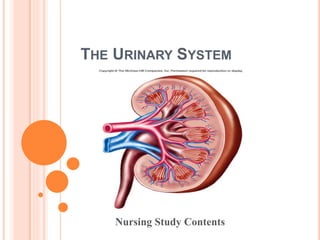
6. REGIONS OF THE KIDNEY
Renal cortex – outer
region
Renal medulla – inside
the cortex
Renal pelvis – inner
collecting tube
Figure 15.2b
7. KIDNEY STRUCTURES
Medullary pyramids – triangular regions of tissue in
the medulla
Renal columns – extensions of cortex-like material
inward
Calyces – cup-shaped structures that funnel urine
towards the renal pelvis
9. NEPHRONS
The structural & functional units of the kidneys
Responsible for forming urine
Main structures of the nephrons
Glomerulus
Renal tubule
11. GLOMERULUS
A specialized
capillary bed
Attached to
arterioles on both sides
(maintains
high pressure)
Large afferent
arteriole
Narrow efferent
arteriole
Figure 15.3c
12. GLOMERULUS
Capillaries are covered with
podocytes from the renal
tubule
The glomerulus sits within a
glomerular capsule (the first
part of the renal tubule)
Figure 15.3c
14. TYPES OF NEPHRONS
Cortical nephrons
Located entirely in the
cortex
Includes most nephrons
Juxtamedullary nephrons
Found at the boundary of
the cortex and medulla
Figure 15.3a
16. FILTRATION
Nonselective passive process
Water and solutes smaller than proteins are forced
through capillary walls
Blood cells cannot pass out to the capillaries
Filtrate is collected in the glomerular capsule and
leaves via the renal tubule
17. REABSORPTION
The peritubular capillaries reabsorb several
materials
Some water
Glucose
Amino acids
Ions
Some reabsorption is passive, most is active
Most reabsorption occurs in the proximal
convoluted tubule
19. SECRETION – REABSORPTION IN REVERSE
Some materials move from the peritubular
capillaries into the renal tubules
Hydrogen and potassium ions
Creatinine
Materials left in the renal tubule move toward the
ureter
21. CHARACTERISTICS OF URINE USED FOR MEDICAL
DIAGNOSIS
Colored somewhat yellow due to the pigment urochrome
(from the destruction of hemoglobin) and solutes
Sterile
Slightly aromatic
Normal pH of around 6
Specific gravity of 1.001 to 1.035
22. URETERS
Slender tubes attaching the kidney to the bladder
Continuous with the renal pelvis
Enter the posterior aspect of the bladder
Runs behind the peritoneum
Peristalsis aids gravity in urine transport
25. URINARY BLADDER WALL
Three layers of smooth muscle (detrusor muscle)
Mucosa made of transitional epithelium
Walls are thick and folded in an empty bladder
Bladder can expand significantly without increasing
internal pressure
26. URETHRA
Thin-walled tube that carries urine from the bladder
to the outside of the body by peristalsis
Release of urine is controlled by two sphincters
Internal urethral sphincter (involuntary)
External urethral sphincter (voluntary)
27. URETHRA GENDER DIFFERENCES
Length
Females – 3–4 cm (1 inch)
Males – 20 cm (8 inches)
Location
Females – along wall of the vagina
Males – through the prostate and penis
Function
Females – only carries urine
Males – carries urine and is a passageway for sperm cells
28. MICTURITION (VOIDING)
Both sphincter muscles must open to allow voiding
The internal urethral sphincter is relaxed after stretching of the
bladder
Activation is from an impulse sent to the spinal cord and then
back via the pelvic splanchnic nerves
The external urethral sphincter must be voluntarily relaxed
29. MAINTAINING WATER BALANCE
Normal amount of water in the human body
Young adult females – 50%
Young adult males – 60%
Babies – 75%
Old age – 45%
Water is necessary for many body functions and levels
must be maintained
30. DISTRIBUTION OF BODY FLUID
Intracellular fluid (inside
cells)
Extracellular fluid (outside
cells)
Interstitial fluid
Blood plasma
Figure 15.8
31. THE LINK BETWEEN
WATER AND SALT
Changes in electrolyte balance causes water to move
from one compartment to another
Alters blood volume and blood pressure
Can impair the activity of cells
32. MAINTAINING WATER BALANCE
Water intake must equal water output
Sources for water intake
Ingested foods and fluids
Water produced from metabolic processes
Sources for water output
Vaporization out of the lungs
Lost in perspiration
Leaves the body in the feces
Urine production
33. MAINTAINING WATER BALANCE
Dilute urine is produced if water intake is excessive
Less urine (concentrated) is produced if large
amounts of water are lost
Proper concentrations of various electrolytes must
be present
34. REGULATION OF WATER AND ELECTROLYTE
REABSORPTION
Regulation is primarily by hormones
Antidiuretic hormone (ADH) prevents excessive water loss in
urine
Aldosterone regulates sodium ion content of extracellular fluid
Triggered by the rennin-angiotensin mechanism
Cells in the kidneys and hypothalamus are active
monitors
35. MAINTAINING ACID-BASE BALANCE IN BLOOD
Blood pH must remain between 7.35 and 7.45 to
maintain homeostasis
Alkalosis – pH above 7.45
Acidosis – pH below 7.35
Most ions originate as byproducts of cellular
metabolism
36. MAINTAINING ACID-BASE BALANCE IN BLOOD
Most acid-base balance is maintained by the
kidneys
Other acid-base controlling systems
Blood buffers
Respiration
37. BLOOD BUFFERS
Molecules react to prevent dramatic changes in hydrogen
ion (H+) concentrations
Three major chemical buffer systems
Bicarbonate buffer system
Phosphate buffer system
Protein buffer system
38. THE BICARBONATE BUFFER SYSTEM
Mixture of carbonic acid (H2CO3) and sodium
bicarbonate (NaHCO3)
Bicarbonate ions (HCO3
–) react with strong acids to
change them to weak acids
Carbonic acid dissociates in the presence of a
strong base to form a weak base and water
39. RESPIRATORY SYSTEM CONTROLS OF ACID-BASE
BALANCE
Carbon dioxide in the blood is converted to
bicarbonate ion and transported in the plasma
Increases in hydrogen ion concentration
produces more carbonic acid
Excess hydrogen ion can be blown off with the
release of carbon dioxide from the lungs
Respiratory rate can rise and fall depending on
changing blood pH
40. RENAL MECHANISMS OF ACID-BASE BALANCE
Excrete bicarbonate ions if needed
Conserve or generate new bicarbonate ions if
needed
Urine pH varies from 4.5 to 8.0
41. DEVELOPMENTAL ASPECTS OF THE URINARY SYSTEM
Functional kidneys are developed by the third
month
Urinary system of a newborn
Bladder is small; urine cannot be concentrated
Control of the voluntary urethral sphincter starts
until age 18 months
Urinary infections are the only common problems
before old age
42. AGING AND THE URINARY SYSTEM
There is a progressive decline in urinary function
The bladder shrinks with aging
Urinary retention is common in males