Downloaded 398 times
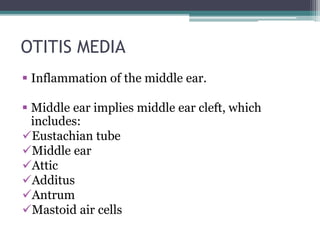
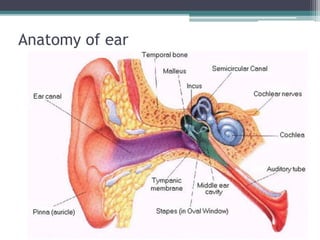
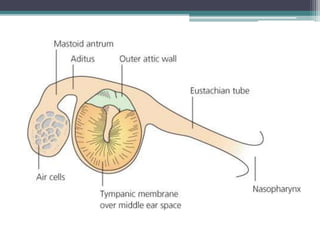
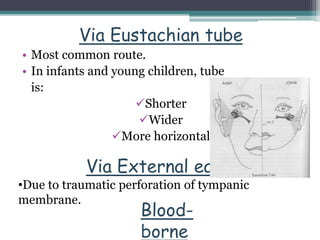

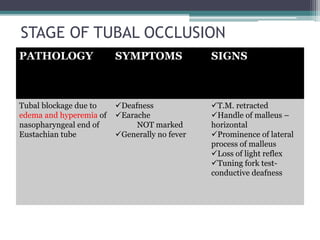
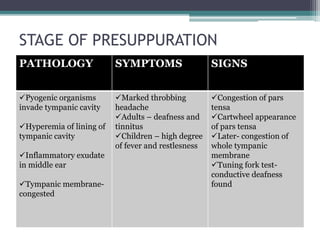
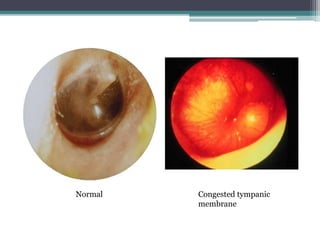
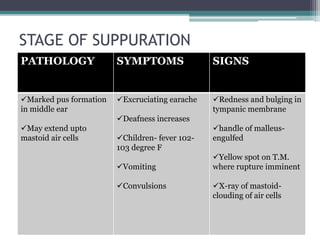
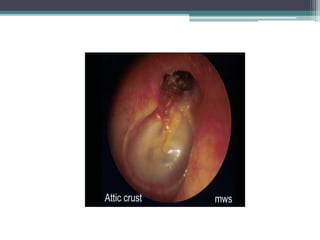
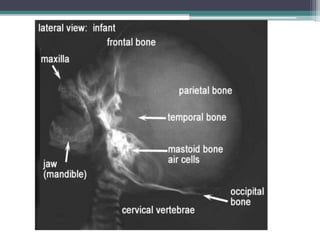
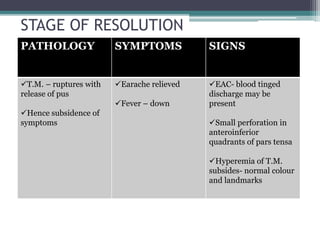
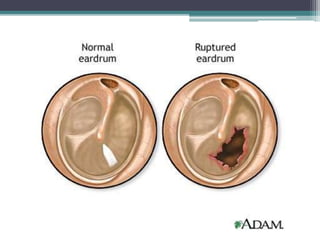
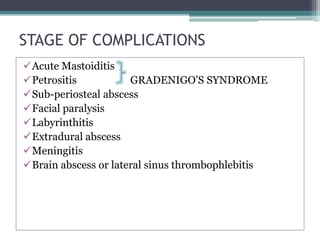
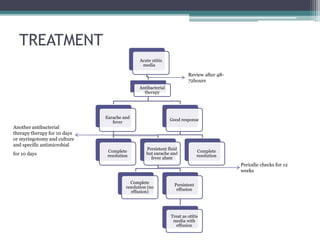


Acute suppurative otitis media is an inflammation of the middle ear caused by bacterial infection, usually following a viral upper respiratory infection. It involves several stages: tubal occlusion from Eustachian tube swelling, presuppuration with bacterial invasion and symptoms like earache, suppuration with pus formation and high fever, resolution upon rupture of the eardrum and drainage of pus, and potential complications like mastoiditis. Treatment involves antibiotics and analgesics; myringotomy may be needed for persistent fluid or complications. Prevention includes childhood vaccines and reducing risk factors like passive smoking.













































































![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)


![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)





![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)
