Downloaded 182 times




![CT, MRI, Bone Scan, and Gallium
Scan
• Imaging studies are not required for most cases of OE. However,
radiologic investigation may be helpful if an invasive infection such as
necrotizing (malignant) OE is suspected or if the diagnosis of
mastoiditis is being considered.
• High-resolution computed tomography (CT) is preferred and better
depicts bony erosion.[6] Radionucleotide bone scanning and gallium
scanning have been used to make the diagnosis. Magnetic resonance
imaging (MRI), though not used as often, may be considered
secondarily or if soft tissue extension is the predominant concern.[7]](https://image.slidesharecdn.com/6-140604043847-phpapp01/85/6-otitis-externa-30-320.jpg)



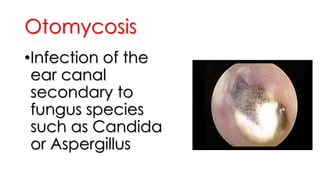
This document provides information about otitis externa (OE), including: 1) OE is an inflammation of the external ear canal caused most often by bacterial infection, but sometimes fungi or viruses. Risk factors include water exposure, trauma from cotton swabs, and eczema. 2) Symptoms include ear pain, fullness, discharge, and hearing loss. Examination reveals erythema and tenderness of the ear canal. 3) Treatment involves cleaning the ear canal and using topical antibiotics, corticosteroids, or antifungals depending on the cause. Imaging is not usually needed but may help identify complications like mastoiditis.











































































































