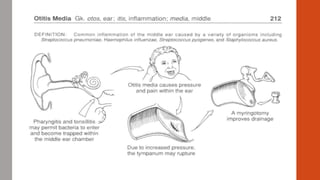
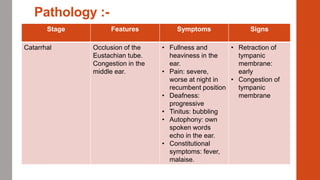
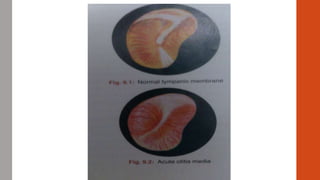
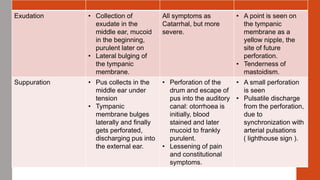
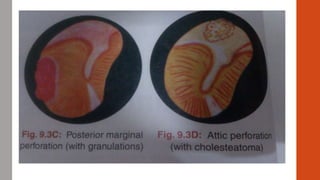
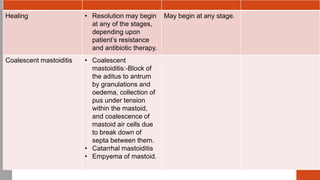
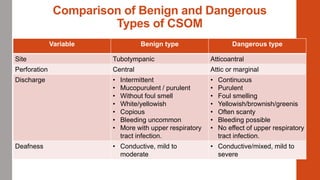
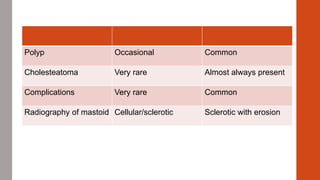
Otitis Media can be acute or chronic. Acute Suppurative Otitis Media is caused by bacterial infection spreading from the nose or throat to the middle ear through the Eustachian tube. It progresses from catarrhal to exudative to suppurative stages, sometimes causing mastoiditis. Chronic Otitis Media can be suppurative or non-suppurative. Chronic Suppurative Otitis Media may be benign or dangerous, with the dangerous type at risk of complications like cholesteatoma. Chronic Non-Suppurative Otitis Media involves non-purulent effusion, causing conditions like serous otitis media and atelectasis. Tuberculous